

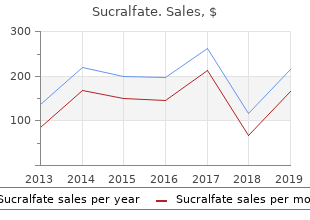
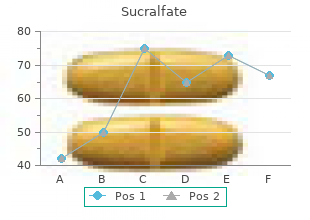
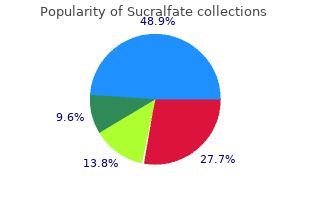
Sucralfate
"Order sucralfate line, gastritis diet ����."
By: Paul Reynolds, PharmD, BCPS
- Critical Care Pharmacy Specialist, University of Colorado Hospital
- Clinical Assistant Professor, Department of Clinical Pharmacy, Skaggs School of Pharmacy and Pharmaceutical Sciences, University of Colorado, Aurora, Colorado

http://www.ucdenver.edu/academics/colleges/pharmacy/Departments/ClinicalPharmacy/DOCPFaculty/Q-Z/Pages/Paul-Reynolds,-PharmD.aspx
Behavioural and cognitive approaches Once a more chronic pattern has established gastritis symptoms flatulence sucralfate 1000mg free shipping, non-pharmacological approaches are more likely to gastritis diet pdf effective sucralfate 1000 mg be effective gastritis and duodenitis definition trusted 1000mg sucralfate. It may be more realistic to gastritis diet ����� order sucralfate online pills suggest avoiding triggers during a known vulnerable period. In long-term follow-up of 9000 Swedish school children with migraine: � One-third had been migraine-free for >1 yr at 6-yr follow-up. Developmental disorders featuring ventriculomegaly/hydrocephalus � Neural tube defects: particularly myelomeningocoele and encephalocoele. Acquired causes of obstructive hydrocephalus � Intraventricular haemorrhage: 80% of premature babies with grade 3 and grade 4 haemorrhages develop progressive ventricular dilatation. Symptoms and signs of hydrocephalus Hydrocephalus may present with acute or chronic symptoms of raised intracranial pressure if it �decompensates�; or asymptomatically. Later childhood � Macrocephaly, may be an isolated nding in arrested hydrocephalus. Shunts � Ventriculo-peritoneal shunts: a proximal catheter in the lateral or 4th ventricle, a distal catheter in the peritoneal cavity. A long length of tube can be placed in the hope of avoiding re-operation between infancy and adulthood, although shunts placed in the neonatal period often fail (typically at about 5�6 yrs age) due to displacement of either the proximal or more commonly the distal catheter tip with growth. Endoscopic 3rd ventriculostomy � For obstructive hydrocephalus particularly due to aqueductal stenosis. Headaches Causes � Over-drainage (exacerbation by upright posture not an entirely sensitive or speci c nding). Other chronic problems � General cognition and speci c de cits (see b �Cognitive disability�, p. Cognitive disability the typical pro le includes good expressive language but weaker compre hension and impaired frontal lobe skills. The former leads to overestimation of cognitive abilities and under-recognition of the latter resulting in �cock tail party syndrome� of ability to �small-talk� but with limited intuitive and empathetic understanding of what is being said. Speci c de cits: attention, short-term memory, reasoning, sequencing actions, mathematics (subcortical information processing de cits). The opening may be subtle (dermal sinus tract) or large (rachischisis), the latter associated with signi cant morbidity and mortality. Spina bi da occulta: implies a developmental vertebral anomaly without overt spinal cord lesion. Generally not included in epidemiological studies of spina bi da, but may share latter�s aetiology. Associated conditions Abnormal development of the spinal cord and ectopic elements � Lipoma: dorsal spinal cord only, or more extensive transitional lesion as in lipomyelomeningocoele. Other malformations outside the spinal cord � 80% of children with myelomeningocoele have hydrocephalus. Environmental insults interact with maternal and embryonic gene mutations and polymorphisms to cause neural tube defects. The disparity is due to termination of pregnancy and in utero deaths, particularly of severe lesions. Assessment of the child with spina bi da As with other complex neurodisability, a multi-disciplinary approach to assessment and management is essential. Early involvement of neuro surgeon, renal, or urological specialist and spinal orthopaedic surgeon required. Neonatal period and early infancy the child may present antenatally or with an unexpected lesion after birth: � Open lesion. Assess muscle bulk, spontaneous anti-gravity movements, spinal re exes, abnormal spread of re exes, and sacral sensation. Neurogenic constipation often present (also effects of concurrent anorectal anomalies). Management with continence advice, regular catheterizations, medication (pro or anti-cholinergics) and surgical procedures (intravesical botulinum toxin and resineferatoxin injections; vesicostomy; bladder augmentation and bladder neck procedures). Treatments include bracing, rigid orthoses, spasticity management, physiotherapy and surgery. Prognosis Ambulation Neurological level of lesion is main predictor of future need for mobility aids and ambulatory ability. Cognitive ability, perceptual disturbance, co ordination, spasticity and bone deformities may impose further limits. Cognition the majority of children with myelomeningocoele do not have overt learning disability. Mortality and morbidity Increased risk of death in infancy with high spinal lesions, open lesions and multiple malformations. Quality of life affected by sequelae and functional limitations rather than level of lesion per se. Tonsillar descent in young children may resolve spontaneously with posterior fossa growth. The association with spina bi da is directly causative: the higher the spinal lesion the more severe the Chiari malformation. Long-term, regular (at least annual) ophthalmological review (particularly of visual elds) is required to detect early signs. In contrast to high pressure headache symptoms are relieved by lying down and worsened by sitting up. Bacterial infection is usually associated with a polymorpho nuclear response in the subarachnoid space; viral, tuberculous and fungal infection causes a lymphocytic response. Meningitis is divided into acute (develops over hours to days) and chronic (days to weeks) forms. Acute bacterial meningitis Incidence and aetiology � the epidemiology is changing as a result of immunization patterns. Pathogenesis � 95% of bacterial meningitides originate from blood-borne dissemination, 5% from local spread. This generates an immune response and an in ammatory cascade killing the bacteria, but also causing brain injury (Table 4. Clinical features � Symptoms: � triad of fever, headache and neck stiffness; � may be associated photophobia and myalgia. If meningococcal infection is suspected, or the child is extremely ill and meningitis is suspected, start treatment prior to investigation. Pneumococcus and HiB can continue to spike temperatures for 7�10 days: consider imaging of the head for effusion/empyema or local abscess formation. If given, they should: � Ideally be administered before the rst antibiotic dose at a dose of 0. Contacts For HiB and meningococcus, with rifampicin at 10 mg/kg for 4 or 2 days, respectively. Fluid restriction may further compromise cerebral circulation, so before restricting uids check plasma and urinary sodium and osmolality, and urine output. Pathogenesis � Primary infection occurs when the tubercle bacillus is inhaled into the lungs and taken up by alveolar macrophages. In the majority of cases, this primary infection passes unnoticed, with only the development of a positive tuberculin skin test to indicate that infection has taken place. Diagnosis is often dif cult to con rm initially, and needs to be based on clinical suspicion. Acetazolamide or ventriculoperitoneal shunting may be used for hydrocephalus (usually communicating). Mortality Mortality is 10�50% depending on stage of presentation; 30% have residual neurological sequelae. Clinical features include headache, fever and neck stiffness fol lowing a prodromal u-like illness. Causative agents Enteroviruses (responsible for 85% of cases) Include echovirus, Coxsackie, poliovirus. All cause diffuse rashes with or without more speci c features: � Echovirus: conjunctivitis, myopathy. Mumps Parotitis, orchitis, pancreatitis with elevated amylase and lipase (extraneural manifestations occur in 50% cases). Features are of developmental stagnation, and later neurological and general cognitive regression with pyramidal signs, hypokinesis and evolving dysphagia and feeding dif culties. In older children, deteriorating school performance, social withdrawal, and emotional lability are seen. May have insidious onset with abnormal behaviour/memory problems that can be mistaken for psy chiatric illness. The former is usually found in the immunocompetent and typically leads to arterial stroke (see b p.
Mixed receptive�expressive language disorders are characterized by de cits in both comprehension and expression of speech [19 gastritis quick relief order genuine sucralfate on-line, 20] gastritis diet ����� buy genuine sucralfate on line. Verbal auditory agnosia or word deafness is characterized by profound impairment in comprehension of spo ken words [18�20 gastritis and duodenitis definition buy sucralfate in united states online, 24] gastritis diet ulcer generic sucralfate 1000 mg mastercard. In phonologic or syntactic de cit dis order, the comprehension or the ability to recognize phonological rules receptively is mostly preserved or is relatively better (in most children) than expression [19, 20, 24]. It is characterized by signi cant omissions, distortions, and substitutions of words, and the speech is telegraphic, with limited vocabulary and grammatical errors. The child tends to use short sentences and has dif culty in repetition of words or sentences [18]. Lexical de cit disorder or lexical�syntactic de cit is characterized by severe de cits in word nding and paraphrasing, jargon, and pseudo-stuttering [19, 20, 24]. There is signi cant de ciency in understanding of connected speech, impoverished syntax, and syntactic distortions. The child may respond to simple commands, and his/her ability to decode wh-questions is limited. Semantic�pragmatic de cit disorder is character ized by poor discourse of connected speech, though the child may apparently be talkative [20]. Other characteristics of this disorder include atypical choices of words, word nding de cits, signi cant de cits in comprehension and verbal reasoning, and tangential and stereotyped speech often with echolalia [20, 24]. Children manifest de cien cies in conversational skills characterized by speaking aloud to no one in particular, poor maintenance of the topic, and responding inaccurately or out of context to commands and questions. Selective mutism is failure to speak in speci c social situations, such as in school, whereas the child is able to speak in other situations such as at home. Twenty to 30% of children with selective mutism have associated articulation problems and language delays. Characterized by errors in articulation and speech sounds, consistent substitution of simple sounds for complex sounds or single consonants for blended consonants, dropped consonants, and errors within words. Problem may not be recognized until preschool Stuttering Disturbed speech uency with atypical rate and rhythm and repetitions of sounds, syllables, words, and phrases generally accompanied by evidence of stress or physical tension. There may be sound prolongations, interjections, pauses within words, and blocking of words. Typical onset between 2 and 7 years with peak at age 5 years Resonance disorders Can be either hypernasal or hyponasal voice due to anatomical factors. Hypernasality may be due to dysfunction of the velopharyngeal mechanism, seen, for example, in cleft palate. Hyponasality is seen, for example, in nasal congestion, upper respiratory infections, nasal anomalies, and hypertrophied adenoids Dysarthria Due to dysfunction of the neuromuscular or motor mechanism for speech production. Characterized mainly by inconsistent misarticulations of speech sounds and words, poor intelligibility, and slow speech Verbal dyspraxia and Both terms describe similar types of largely speech production speech programming problems. These disorders may signi cantly in uence expressive disorder language as well Regression of Previously Acquired Skills or Failure to Acquire Expected New Skills Main causes of developmental regression include autistic regression, Rett syn drome, childhood disintegrative disorder, and Landau�Kleffner syndrome [4, 18]. Rett syndrome demonstrates loss of developmental milestones after a period of normal development, autistic behaviors, characteristic abnormal wringing hand movements, and a deceleration in head circumference [4]. Following early regres sion there is some recovery, but then stagnation and late motor deterioration ensue. Some of the other features in children with Rett syndrome include hyperventilation, breath holding, air swallowing, bruxism, gait dyspraxia, neurogenic scoliosis, auto nomic dysfunction, inappropriate laughing and screaming spells, and intense eye communication. It has very high male predominance, and the typical onset is between 3 and 4 years of age. The much later onset of loss of skills after a period of normal development differentiates it from Rett disorder. Less common causes of progressive encephalopathy with developmental regres sion with onset after 2 years of age include genetic/metabolic lysosomal storage disease; disorders of gray matter such as ceroid lipofuscinosis and mitochondrial disorders; white matter diseases such as adrenoleukodystrophy, Alexander disease, acquired human immunode ciency syndrome encephalopathy, and post-infectious subacute sclerosing panencephalitis [4]. Early Learning Dif culties and Behavioral Symptoms Early (about third-grade) academic or learning dif culties can present as poor grades, delay in completing assignments, inattention, delay in learning new skills, and dif culties in comprehending or reading [36, 37]. These children may also be shy and withdrawn and have behavioral problems at school. Differential diag nosis should include attention-de cit/hyperactivity disorder, sensory impairments, speci c learning disability, developmental coordination disorder, and intellectual disability or borderline intellectual functioning [36]. Vision and hearing impairment may be associated with other developmental dis abilities. A child with visual impairment might close or cover one eye; squint the eyes or frown; complaint that things are blurry or hard to see; have trouble reading or doing other close-up work or hold objects close to eyes; blink more than usual or seem cranky when doing close-up work such as looking at a book. A child with complete or partial hearing impairment might not turn to the source of a sound from birth to 3 or 4 months of age; may not say single words, such as �dada� or �mama� by 1 year of age; and turn head when he/she sees you but not if you only call out his/her name. Developmental coordination disorder affects school-age children and persists into adolescent years. Dif culties in motor coordination will cause substantial impairment in academic function or activities of daily living. Earliest manifesta tions may include dif culty in sucking and swallowing, drooling during infancy, speech dif culties, and delayed motor milestones during early childhood. Parents may observe that the child has dif culties with many of the ne motor tasks such as using scissors, tying shoe laces, or buttoning or unbuttoning. They also may drop objects, have poor handwriting, or will frequently bump into furniture or other people. Adolescents Academic Dif culties Developmental learning disabilities or disorders are the main consideration in older children and adolescents with dif culties with school work [36�51]. In addition to 2 Basic Concepts of Developmental Diagnosis 23 speci c signs associated with learning disorders, these children may present with behavioral problems. Developmental learning disorder is diagnosed when the child�s or adolescent�s scores on an individually administered standardized achievement test (in reading, mathematics, or written expression) are substantially below that expected based on his/her age, education, and level of intelligence (on individually administered stan dardized tests) [36, 37]. Some of the clinical fea tures of reading disorder include delayed language, problems with rhyming words or words that sound alike, dif culty in learning letters of the alphabet, spelling errors, dif culty in reading (decoding) unfamiliar or nonsense words or single words, and slow reading [38�41]. Children with mathematics disorder will demonstrate problems with skills in arithmetic by the end of second or third grade [42�48]. Some of the features include dif culties understanding or naming mathematical terms, operations, or concepts; dif culties decoding or recognizing mathematical symbols or signs; dif culties copying numbers or gures, following sequences of mathematical steps, counting, or multiplication tables [42�48]. Disorder of written expression is apparent by the end of the fth grade and manifests problems with writing skills, which include grammatical errors, punctuation errors, poor paragraph organization, spelling errors, and very poor handwriting [47, 48]. Non-verbal learning disability demonstrates dif culties with problem-solving, visual�spatial, and visual�perceptual de cits, while the language-based skills and intelligence are normal [47]. Diagnosis A detailed prenatal, birth, perinatal, neonatal, and developmental history is the most essential aspect in the diagnostic evaluation of children with atypical devel opment. In infants, examination should focus on neurological and developmental assessment. The examination should document serial measurements of height, weight, and head circumference on appropriate graphs. Also a meticulous search of dysmorphic fea tures or congenital anomalies should be an integral component of the examination. In addition, in adolescents the examination should include assessment of Tanner stage and mental status examination. Any parental concern about development, hearing, or vision is an indication for further evaluation of developmental or sensory problems. Hearing evaluation is mandatory in all children with symptoms or signs of developmental disorder. Current guidelines recommend universal hearing screening by 1 month of age with subsequent diagnostic audiological testing completed by 3 months of age. Vision screening should be part of periodic health maintenance examinations in all children. Developmental screening with appropriate standardized screening instrument (see Table 2. If there is no periodic health maintenance exam at 30 months, then perform it at 24 months of age [5]. If of ce screening yields suspicion for a developmental disorder, a more for mal and advanced testing is necessary. Consider neuroimaging, electroencephalography, tests for genetic disorders, and speci c laboratory tests for metabolic disorders based on history, examination, and consultation with appropriate medical specialists [5, 6, 8, 9, 52] (Table 2. Conclusions Developmental progression is generally described in four main domains, namely motor, speech�language, social�emotional, and cognitive.
Buy 1000 mg sucralfate mastercard. 8 Facts about Irritable Bowel Syndrome | Stomach Problems.
A 60-second intravaginal ejaculatory latency time is an appropriate cutoff for the diagnosis of lifelong premature (early) ejaculation in heterosexual men gastritis diet x factor buy cheap sucralfate on-line. There are insufficient data to gastritis treatment diet buy sucralfate 1000 mg line determine if this duration criterion can be applied to gastritis diet ���� buy sucralfate 1000mg ac� quired premature (early) ejaculation gastritis diet ��������� buy on line sucralfate. The durational definition may apply to males of varying sexual orientations, since ejaculatory latencies appear to be similar across men of different sexual orientations and across different sexual activities. Associated Features Supporting Diagnosis Many males with premature (early) ejaculation complain of a sense of lack of control over ejaculation and report apprehension about their anticipated inability to delay ejaculation on future sexual encounters. The following factors may be relevant in the evaluation of any sexual dysfunction: 1) partner factors. Prevaience Estimates of the prevalence of premature (early) ejaculation vary widely depending on the definition utilized. Internationally, more than 20%-30% of men ages 18-70 years report concern about how rapidly they ejaculate. Some men may experience premature (early) ejaculation during their initial sexual encounters but gain ejaculatory control over time. It is the persis� tence of ejaculatory problems for longer than 6months that determines the diagnosis of pre� mature (early) ejaculation. In contrast, some men develop the disorder after a period of having a normal ejaculatory latency, known as acquired premature (early) ejaculation. There is far less known about acquired premature (early) ejaculation than about lifelong premahire (early) ejaculation. The acquired form likely has a later onset, usually appearing during or af� ter the fourth decade of life. Reversal of medical conditions such as hyperthyroidism and prostatitis appears to restore ejaculatory latencies to baseline values. In approximately 20% of men with premature (early) ejacu� lation, ejaculatory latencies decrease further with age. Age and relationship length have been found to be negatively associated with prevalence of premature (early) ejaculation. Premature (early) ejaculation may be more common in men with anx� iety disorders, especially social anxiety disorder (social phobia). There is a moderate genetic contribution to lifelong prema� ture (early) ejaculation. Premature (early) ejaculation may be associated with dopamine transporter gene polymorphism or serotonin transporter gene polymorphism. Thyroid disease, prostatitis, and drug withdrawal are associated with acquired premature (early) ejaculation. Positron emission tomography measures of regional cerebral blood flow dur� ing ejaculation have shown primary activation in the mesocephalic transition zone, includ� ing the ventral tegmental area. C uiture-R elated Diagnostic issues Perception of what constitutes a normal ejaculatory latency is different in many cultures. Such differences may be ex� plained by cultural or religious factors as well as genetic differences between populations. Gender-Reiated Diagnostic Issues Premature (early) ejaculation is a sexual disorder in males. Males and their sexual partners may differ in their perception of what constitutes an acceptable ejaculatory latency. There may be increasing concerns in females about early ejaculation in their sexual partners, which may be a reflection of changing societal attitudes concerning female sexual activity. Diagnostic iViarlcers Ejaculatory latency is usually monitored in research settings by the sexual partner utilizing a timing device. For vaginal intercourse, the time between intravaginal penetration and ejaculation is measured. Functional Consequences of Prem ature (Eariy) Ejaculation A pattern of premature (early) ejaculation may be associated with decreased self-esteem, a sense of lack of control, and adverse consequences for partner relationships. It may also cause personal distress in the sexual partner and decreased sexual satisfaction in the sexual partner. Ejaculation prior to penetration may be associated with difficulties in conception. When problems with premature ejaculation are due exclusively to substance use, intoxication, or withdrawal, substance/ medication-induced sexual dysfunction should be diagnosed. It is necessary to identify males with normal ejaculatory latencies who desire longer ejaculatory latencies and males who have episodic premature (early) ejaculation. Neither of these situations would lead to a diagnosis of premature (early) ejaculation, even though these situations may be distressing to some males. Comorbidity Premature (early) ejaculation may be associated with erectile problems. In many cases, it may be difficult to determine which difficulty preceded the other. Lifelong premature (early) ejaculation may be associated with certain anxiety disorders. Acquired premature (early) ejaculation may be associated with prostatitis, thyroid disease, or drug withdrawal. A clinically significant disturbance insexual function is predominant inthe clinical picture. The disturbance is not better explained by a sexual dysfunction that is not substance/ medication-induced. Such evidence of an independent sexual dysfunction could in� clude the following: the symptoms precede the onset of the substance/medication use; the symptoms persist for a substantial period of time. Note: this diagnosis should be made instead of a diagnosis of substance intoxication or substance withdrawal only when the symptoms in Criterion A predominate in the clinical picture and are sufficiently severe to warrant clinical attention. If a mild substance use disorder is comorbid with the substance induced sexual dysfunction, the 4th position character is �1,�and the clinician should record �mild [substance] use disorder�before the substance-induced sexual dysfunction. With onset during withdrawai: If criteria are met for withdrawal from the substance and the symptoms develop during, or shortly after, withdrawal. With onset after medication use: Symptoms may appear either at initiation of medi� cation or after a modification or change in use. Specify current severity: Mild: Occurs on 25%-50% of occasions of sexual activity. The name of the substance/medication-induced sexual dysfunction begins with the specific substance. For example, in the case of erectile dysfunction occurring during intoxication in a man with a severe alcohol use disorder, the diagnosis is 291. When more than one substance is judged to play a sig nificant role in the development of the sexual dysfunction, each should be listed separately. When recording the name of the disorder, the comorbid substance use disorder (if any) is listed first, followed by the word "with," followed by the name of the substance-induced sexual dysfunction, followed by the specification of onset. For example, in the case of erectile dysfunction occur� ring during intoxication in a man with a severe alcohol use disorder, the diagnosis is F10. If the substance-induced sexual dysfunction occurs without a co� morbid substance use disorder. When more than one substance is judged to play a significant role in the development of the sexual dysfunction, each should be listed separately. Diagnostic Features the major feature is a disturbance in sexual function that has a temporal relationship with substance/medication initiation, dose increase, or substance/medication discontinuation. Associated Features Supporting Diagnosis Sexual dysfunctions can occur in association with intoxication with the following classes of substances: alcohol; opioids; sedatives, hypnotics, or anxiolytics; stimulants (including co� caine); and other (or unknown) substances. Sexual dysfunctions can occur in association with withdrawal from the following classes of substances: alcohol; opioids; sedatives, hyp� notics, or anxiolytics; and other (or unknown) substances. Medications that can induce sex� ual dysfunctions include antidepressants, antipsychotics, and hormonal contraceptives. The most commonly reported side effect of antidepressant drugs is difficulty with or� gasm or ejaculation. Certain agents, such as bupropion and mirtazapine, appear not to be associated with sexual side effects.
Often argues with authority figures or gastritis diet amazon discount sucralfate 1000mg without prescription, for children and adolescents gastritis diet 9000 buy generic sucralfate canada, with adults gastritis earth clinic order 1000 mg sucralfate mastercard. Often actively defies or refuses to gastritis dietitian buy sucralfate 1000 mg free shipping comply with requests from authority figures or with rules. Note: the persistence and frequency of these behaviors should be used to distinguish a behavior that is within normal limits from a behavior that is symptomatic. For children younger than 5 years, the behavior should occur on most days for a period of at least 6 months unless otherwise noted (Criterion A8). While these frequency criteria provide guidance on a minimal lev� el of frequency to define symptoms, other factors should also be considered, such as whether the frequency and intensity of the behaviors are outside a range that is nor� mative for the individual�s developmental level, gender, and culture. The disturbance in behavior is associated with distress inthe individual or others in his or her immediate social context. The behaviors do not occur exclusively during the course of a psychotic, substance use, depressive, or bipolar disorder. Specifiers It is not uncommon for individuals with oppositional defiant disorder to show symptoms only at home and only with family members. However, the pervasiveness of the symp� toms is an indicator of the severity of the disorder. Diagnostic Features the essential feature of oppositional defiant disorder is a frequent and persistent pattern of angry/irritable mood, argumentative/defiant behavior, or vindictiveness (Criterion A). It is not unusual for individuals with oppositional defiant disorder to show the behav� ioral features of the disorder without problems of negative mood. However, individuals with the disorder who show the angry/irritable mood symptoms typically show the be� havioral features as well. The symptoms of oppositional defiant disorder may be confined to only one setting, and this is most frequently the home. Individuals who show enough symptoms to meet the diagnostic threshold, even if it is only at home, may be significantly impaired in their social functioning. However, in more severe cases, the symptoms of the disorder are pres� ent in multiple settings. Because these behaviors are common among siblings, they must be observed during interactions with persons other than siblings. Also, because symptoms of the disorder are typically more evident in interactions with adults or peers whom the individual knows well, they may not be apparent during a clinical examination. The symptoms of oppositional defiant disorder can occur to some degree in individu� als without this disorder. There are several key considerations for determining if the be� haviors are symptomatic of oppositional defiant disorder. First, the diagnostic threshold of four or more symptoms within the preceding 6months must be met. For example, it is not unusual for preschool children to show temper tantrums on a weekly basis. Temper outbursts for a preschool child would be considered a symptom of oppositional defiant disorder only if they occurred on most days for the preceding 6months, if they occurred with at least three other symptoms of the dis� order, and if the temper outbursts contributed to the significant impairment associated with the disorder. The symptoms of the disorder often are part of a pattern of problematic interactions with others. Furthermore, individuals with this disorder typically do not regard themselves as angry, oppositional, or defiant. Instead, they often justify their behavior as a response to unreasonable demands or circumstances. Thus, it can be difficult to disentangle the rela� tive contribution of the individual with the disorder to the problematic interactions he or she experiences. Whether or not the clinician can separate the relative contributions of potential causal factors should not influence whether or not the diagnosis is made. In the event that the child may be living in particularly poor conditions where neglect or mistreatment may occur. Associated Features Supporting Diagnosis In children and adolescents, oppositional defiant disorder is more prevalent in families in which child care is disrupted by a succession of different caregivers or in families in which harsh, inconsistent, or neglectful child-rearing practices are common. Oppositional defiant disorder has been associated with increased risk for suicide attempts, even after comorbid disorders are controlled for. Prevaience the prevalence of oppositional defiant disorder ranges from 1% to 11%, with an average prevalence estimate of around 3. The rate of oppositional defiant disorder may vary depending on the age and gender of the child. This male predominance is not consistently found in samples of adolescents or adults. Development and Course the first symptoms of oppositional defiant disorder usually appear during the preschool years and rarely later than early adolescence. Oppositional defiant disorder often precedes the development of conduct disorder, especially for those with the childhood-onset type of conduct disorder. However, many children and adolescents with oppositional defiant disorder do not subsequently develop conduct disorder. Oppositional defiant disorder also conveys risk for the development of anxiety disorders and major depressive disorder, even in the absence of conduct disorder. The defiant, argumentative, and vindictive symp� toms carry most of the risk for conduct disorder, whereas the angry-irritable mood symp� toms carry most of the risk for emotional disorders. Children and adolescents with oppositional defiant disorder are at increased risk for a number of prob� lems in adjustment as adults, including antisocial behavior, impulse-control problems, substance abuse, anxiety, and depression. Many of the behaviors associated with oppositional defiant disorder increase in fre� quency during the preschool period and in adolescence. Thus, it is especially critical dur� ing these development periods that the frequency and intensity of these behaviors be evaluated against normative levels before it is decided that they are symptoms of opposi� tional defiant disorder. Harsh, inconsistent, or neglectful child-rearing practices are common in families of children and adolescents with oppositional defiant disorder, and these parent� ing practices play an important role in many causal theories of the disorder. However, the vast majority of studies have not separated children with oppositional de� fiant disorder from those with conduct disorder. Thus, it is unclear whether there are markers specific to oppositional defiant disorder. Culture-R elated Diagnostic Issues the prevalence of the disorder in children and adolescents is relatively consistent across countries that differ in race and ethnicity. Functional Consequences of Oppositional Defiant Disorder When oppositional defiant disorder is persistent throughout development, individuals with the disorder experience frequent conflicts with parents, teachers, supervisors, peers, and romantic partners. Conduct disorder and oppositional defiant disorder are both related to conduct problems that bring the individual in conflict with adults and other authority figures. The behaviors of oppositional defiant disorder are typically of a less severe nature than those of conduct disorder and do not include ag� gression toward people or animals, destruction of property, or a pattern of theft or deceit. Furthermore, oppositional defiant disorder includes problems of emotional dysregulation. Depressive and bipolar disorders often involve neg� ative affect and irritability. As a result, a diagnosis of oppositional defiant disorder should not be made if the symptoms occur exclusively during the course of a mood disorder. Oppositional defiant disorder shares with dis� ruptive mood dysregulation disorder the symptoms of chronic negative mood and temper outbursts. However, the severity, frequency, and chronicity of temper outbursts are more severe in individuals with disruptive mood dysregulation disorder than in those with oppositional defiant disorder. Thus, only a minority of children and adolescents whose symptoms meet criteria for oppositional defiant disorder would also be diagnosed with dis� ruptive mood dysregulation disorder. When the mood disturbance is severe enough to meet criteria for disruptive mood dysregulation disorder, a diagnosis of oppositional defiant dis� order is not given, even if all criteria for oppositional defiant disorder are met. However, individuals with this disorder show serious aggression toward others that is not part of the definition of oppositional defiant disorder. In individuals with intel� lectual disability, a diagnosis of oppositional defiant disorder is given only if the opposi� tional behavior is markedly greater than is commonly observed among individuals of comparable mental age and with comparable severity of intellectual disability. Oppositional defiant disorder must also be distinguished from a failure to follow directions that is the result of impaired language comprehension. Oppositional defiant disorder must also be dis� tinguished from defiance due to fear of negative evaluation associated with social anxiety disorder.