

Levonorgestrel Bp
"Purchase line levonorgestrel, birth control for menopause."
By: Randolph E. Regal, BS, PharmD
- Clinical Associate Professor, Department of Clinical Pharmacy, College of Pharmacy, University of Michigan
- Clinical Pharmacist, University of Michigan Health System, Ann Arbor, Michigan

https://pharmacy.umich.edu/people/reregal
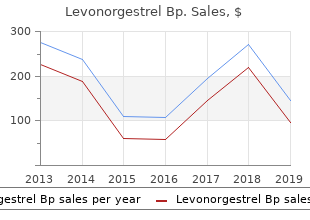
Within one week birth control pills buy online buy levonorgestrel 0.18mg low cost, 92% to birth control pills after sex purchase levonorgestrel discount 98% of the dose was recovered missed birth control pill 6 hours discount 0.18mg levonorgestrel free shipping, almost entirely in the urine birth control dangers purchase 0.18 mg levonorgestrel visa. Gemcitabine (<10%) and the inactive uracil metabolite, 2 deoxy-2,2 difluorouridine (dFdU) accounted for 99% of the excreted dose. Specific Populations Geriatric Patients 17 Clearance of gemcitabine was affected by age. The lower clearance in geriatric patients results in higher concentrations of gemcitabine for any given dose. Differences in either clearance or volume of distribution based on patient characteristics or the duration of infusion result in changes in half-life and plasma concentrations. Table 15 shows plasma clearance and half-life of gemcitabine following short infusions for typical patients by age and sex. Table 15: Gemcitabine Clearance and Half-Life for the �Typical� Patient a a Age Clearance Men Clearance Women Half-Life Men Half-Life Women 2 2 (L/hr/m) (L/hr/m) (min) (min) 29 92. Gemcitabine half-life for short infusions ranged from 42 to 94 minutes and for long infusions varied from 245 to 638 minutes, depending on age and sex, reflecting a greatly increased volume of distribution with longer infusions. Male and Female Patients Females have lower clearance and longer half-lives than male patients as described in Table 15. Patients with Renal Impairment No clinical studies have been conducted with gemcitabine in patients with decreased renal function. Patients with Hepatic Impairment No clinical studies have been conducted with gemcitabine in patients with decreased hepatic function. Gemcitabine was mutagenic in an in vitro mouse lymphoma (L5178Y) assay and was clastogenic in an in vivo mouse micronucleus assay. In female mice, fertility was not affected but maternal toxicities were observed at 1. There was no significant difference in overall survival between the treatment arms. Demographic and baseline characteristics were similar between treatment arms (Table 18). Figure 2: Kaplan-Meier Curves for Time to Documented Disease Progression in Study 2 14. The major efficacy outcome measure in both trials was �clinical benefit response�. A patient was considered to have had a clinical benefit response if either of the following occurred: � the patient achieved a 50% reduction in pain intensity (Memorial Pain Assessment Card) or analgesic consumption, or a 20-point or greater improvement in performance status (Karnofsky Performance Status) for a period of at least 4 consecutive weeks, without showing any sustained worsening in any of the other parameters. Sustained worsening was defined as 4 consecutive weeks with either any increase in pain intensity or analgesic consumption or a 20-point decrease in performance status occurring during the first 12 weeks of therapy. Demographics and baseline characteristics were similar between the arms (Table 22). Instruct patients to immediately contact their healthcare provider should any signs or symptoms of infection, including fever, or if bleeding or signs of anemia, occur [see Warnings and Precautions (5. Pulmonary Toxicity Advise patients of the risks of pulmonary toxicity, including respiratory failure and death. Instruct patients to immediately contact their healthcare provider for development of shortness of breath, wheezing, or cough [see Warnings and Precautions (5. Hemolytic Uremic Syndrome and Renal Failure Advise patients of the risks of hemolytic uremic syndrome and associated renal failure. Instruct patients to immediately contact their healthcare provider for changes in the color or volume of urine output or for increased bruising or bleeding [see Warnings and Precautions (5. Hepatic Toxicity Advise patients of the risks of hepatic toxicity including liver failure and death. Instruct patients to immediately contact their healthcare provider for signs of jaundice or for pain/tenderness in the right upper abdominal quadrant [see Warnings and Precautions (5. Rational: Does the intervention meet the test of competent assessment (diagnosis) and scientifically proven benefit Do you ever require an Eye opener (ie, drink of alcohol) to get going in the morning Other pathological causes should be excluded by clinical history, focused examination and P investigations. Inpatient management should be considered if there is at least one of the following: P G continued nausea and vomiting and inability to keep down oral antiemetics G continued nausea and vomiting associated with ketonuria and/or weight loss (greater than 5% of body weight), despite oral antiemetics G confirmed or suspected comorbidity (such as urinary tract infection and inability to tolerate oral antibiotics). Combinations of different drugs should be used in women who do not respond to a single antiemetic. Clinicians should use antiemetics with which they are familiar and should use drugs from different B classes if the first drug is not effective. Metoclopramide is safe and effective, but because of the risk of extrapyramidal effects it should be B used as second-line therapy. There is evidence that ondansetron is safe and effective, but because data are limited it should be C used as second-line therapy. C Corticosteroids Corticosteroids should be reserved for cases where standard therapies have failed. B What is the best rehydration regimen for ambulatory daycare and inpatient management Dextrose infusions are not appropriate unless the serum sodium levels are normal and thiamine D has been administered. A Acustimulations � acupressure and acupuncture Women may be reassured that acustimulations are safe in pregnancy. Urea and serum electrolyte levels should be checked daily in women requiring intravenous fluids. P Histamine H2 receptor antagonists or proton pump inhibitors may be used for women developing D gastro-oesophageal reflux disease, oesophagitis or gastritis. When should enteral and parenteral nutrition be considered and what are the risks to the mother and fetus When all other medical therapies have failed, enteral or parenteral treatment should be considered D with a multidisciplinary approach. All therapeutic measures should have been tried before offering termination of a wanted pregnancy. It gives advice for multidisciplinary professionals involved in the care of women with these conditions, including how to counsel and support women before, during and after their pregnancies. Search terms included �nausea and vomiting�, �vomiting�, �nausea�, �hyperemesis�, �morning sickness�, �antiemetic agent�, �fluids� and �hydration�. Further information about the assessment of evidence and the grading of recommendations may be found in Appendix I. It typically starts between the fourth and seventh weeks of Evidence gestation, peaks in approximately the ninth week and resolves by the 20th week in 90% of level 2� women. What initial clinical assessment and baseline investigations should be done before deciding on treatment Bilirubin levels can be slightly raised but without Evidence jaundice, and amylase levels can be mildly raised too. An ultrasound scan should be scheduled to confirm viability and gestational age and to rule out multiple pregnancy or trophoblastic disease. Other pathological causes of nausea and vomiting include peptic ulcers, cholecystitis, gastroenteritis, hepatitis, pancreatitis, genitourinary conditions such as urinary tract infection Evidence or pyelonephritis, metabolic conditions, neurological conditions and drug-induced nausea and level 3 vomiting. If women are unable to tolerate oral antiemetics or oral fluids then ambulatory daycare management, which provides parenteral fluids, parenteral vitamins (multi and B-complex)30 and antiemetics, is appropriate if local resources allow. Ambulatory daycare management has been successfully and safely set up in units and is associated with high patient satisfaction. Drug-induced B extrapyramidal symptoms and oculogyric crises can occur with the use of phenothiazines and metoclopramide. These drugs include: Evidence antihistamines (histamine H1 receptor antagonists) such as promethazine, cyclizine, cinnarizine, level 2++ doxylamine37 and dimenhydrinate; phenothiazines including prochlorperazine, chlorpromazine and perphenazine; and dopamine antagonists including metoclopramide38 and domperidone. Because different drug classes may have different mechanisms of action and therefore synergistic effects, combinations of drugs from different classes should be used in women who do not respond to a single antiemetic. Furthermore, persistent vomiting may mean that oral doses of antiemetics are not absorbed and therefore the intravenous, rectal, subcutaneous or intramuscular routes may be necessary and more effective. Due to the risk of extrapyramidal effects with metoclopramide it should be used as second-line therapy. A review of metoclopramide,39 conducted by the European Medicines Agency�s Committee for Medicinal Products for Human Use, has confirmed the risks of short-term extrapyramidal disorders and tardive dyskinesia, particularly in young people.
A persistent preoccupation with (Criterion removed or possibly subsumed into parts of objects B3) B4 birth control and womens rights movement purchase 0.18 mg levonorgestrel free shipping. Symptoms must be present in early childhood (but may not fully manifest until social demands exceed limited capacities) D birth control online buy levonorgestrel 0.18mg cheap. Screening and diagnosis therefore depend upon behavioural observation within conceptual frameworks that are reflected in the structure of different tools birth control quick start algorithm order levonorgestrel 0.18 mg with visa. It is evident that appropriately developed tools guide observation and history taking birth control for women-0ver50-weding-party-dress generic levonorgestrel 0.18 mg without a prescription, allowing earlier, more reliable and repeatable assessment. A range of tools with different characteristics exist for both screening/surveillance and diagnosis. This topic was broken down into specific questions on each identified tool as follows: 1. The search strategy is outlined in the report that was submitted to the Ministry of Health. In summary, a comprehensive number of online bibliographic databases, review and evidence-based databases, library catalogues and international government health websites were searched using a variety of search terms, together with related words, around the themes of �differential diagnosis�, �questionnaires�, �sensitivity and specificity� and �autism�. Abstracts and/or titles (where the abstract was not available) from the resulting 327 items were scanned for relevance. Articles were selected on the basis of relevance to answering the 302 New Zealand Autism Spectrum Disorder Guideline Appendices above questions. Articles relating to adults, pilot studies, short reports or tools that were not developed or available in English were eliminated from consideration. During the process of selection of evidence, an important review was identified, that had analysed systematically all relevant evidence (2750 articles) published up to 1998. It was decided to accept this review as a definitive summary of all evidence before 1998. Twenty-one additional relevant studies were identified from the search from 1998 onwards. It is a comprehensive structured parent interview which takes one hour to deliver, with specific training and validation procedures. This is a structured interview and observations with 15 items, designed for children > 24 months, which takes 30�45 minutes to deliver. B New Zealand Autism Spectrum Disorder Guideline 303 Appendices There are several other tools under development, some of which are mentioned in the American Practice Parameter45 but which have not yet achieved wide acceptance. Note: Screening instruments are generally less expensive, less time consuming and require less training than diagnostic tools. Can the tool be used without modification with Maori, Pacific and Asian individuals No autism-specific screening or diagnostic tool has been validated in either the New Zealand or Australian settings. Although some tools reported in the English language literature have been adapted and utilised in Chinese and in Japanese populations, no reports exist of studies in Maori or Pacific populations. This represents a clear opportunity for New Zealand to do this work as a part of the internal audit of the guideline. Recommendations: Grade Experienced clinicians are usually necessary for accurate and appropriate diagnosis B of autism. Comprehensive multidisciplinary assessment is recommended as being most B important for autism diagnosis compared with other developmental disabilities. How does the cost of using the tool compare with other methods including experienced clinician assessment Cost analysis was not a part of the search strategy for this literature review so no formal answer is possible. However, it is unlikely that there are any cost analyses comparing diagnostic tools with clinician assessment in the literature. Different tools have been compared with each other yielding kappa scores for agreement from as low as 0. A bibliography was prepared by the Clearing House for Health Outcomes and Health Technology Assessment in March 2004 at the direction of Lester Mundell, Chief Advisor, Disability Support Services, Ministry of Health. The search strategy is outlined in the report submitted to the Ministry of Health. In summary, a comprehensive number of online bibliographic databases, review and evidence-based databases, library catalogues and international government health websites were searched using a variety of search terms (together with related words) around the themes of �cognitive�, �diagnosis� and �autism�. Abstracts and/or titles (where abstracts were not available) from the identified studies (n = 183) were analysed and given a preliminary grading on the basis of the likely degree of relevance in terms of capacity to answer the above questions. The selected articles are included in evidence tables with the following relevance grading: Highly relevant (n=18) Probably relevant (n=36) Possibly relevant (n=23) Not relevant (n=106) the 77 articles selected as being relevant were obtained through online and available library sources. Of the above articles or publications, 15 of the Highly Relevant (83%), 19 of the Probably Relevant (53%) and 11 of the Possibly Relevant (52%) were obtained. The list and abstracts of those not obtained were peer reviewed by a subgroup of the Guideline Development Team, and a decision was made to seek a further four articles. The analysed articles had a number of different study designs: reviews, guidelines, cohort studies (of groups of �higher functioning� autistic children who had cognitive tests at baseline and at follow-up) and studies of cognitive differences and styles in autism versus controls (either normal peers or those with intellectual or language difficulties). Relevant cohort and case control studies were reviewed using an evidence template. New Zealand Autism Spectrum Disorder Guideline 305 Appendices Conclusions Grade There are particular patterns of skills and weaknesses on formal tests of cognition A associated with autism (but none are so specific that they significantly contribute to the clinical diagnosis). Specific underlying cognitive deficits are postulated to be at the core of the C symptoms observed (theory of mind deficit, executive function deficit, weak central coherence). Recommendation: Grade Formal baseline cognitive and/or developmental assessment is recommended at B diagnosis. There is no evidence for or against this, but there is good evidence it allows better prediction of prognosis. There is no evidence for or against this, but extrapolation from studies supports the conclusion that better definition of learning skills and prognosis by cognitive assessment will assist planning optimal intervention. Expert supporting opinion from the studies can be summarised as follows: (a) Cognition is not part of the clinical criteria for autism but it is an important variable that influences diagnosis, is related to associated medical disabilities (such as epilepsy), and predicts outcome. Measures of nonverbal problem solving in �high functioning� individuals with autism correlate with outcome (whereas) the severity of autistic behaviours is a poor predictor of prognosis. Cognitive ability also has an important role in prognosis and intervention planning. An estimation of potential is necessary for the following reasons: 306 New Zealand Autism Spectrum Disorder Guideline Appendices Functioning level, which includes cognitive and adaptive evaluation, is important for differential diagnosis and intervention planning. It is also extremely difficult to document significant social and communicative deficits below this age level. This, of course, is dependent upon the relative degree of certainty with which cognitive impairment can be established. Considerations and barriers at two age levels (roughly equating to primary and secondary) are summarised in the accompanying text boxes. Individualised supports and services this element includes incorporating a focus on the child�s strengths and weaknesses, as well as family preferences, and the child and young person preferences and interests to determine the most appropriate intensity and level of instruction to meet their individual goals. Therefore, learning objectives for teaching in almost teachers should: any curriculum area in the primary area. Individual attention to the child�s needs to determine intensity and level of instruction Provide professional learning and development for teachers so they are skilled and knowledgeable enough to make assessments to determine the student�s needs and priorities. Specialists and teachers need skills in Students do not need a goal for every subject. Goals At a certain point, adaptive behaviours may need to be carefully thought out and need to become the priority. They may need to do fewer understand the purpose and the steps subjects than other students and have study towards attaining the goals. Systematic instruction this involves carefully planning for instruction by identifying valid educational goals, carefully outlining instructional procedures for teaching, implementing the procedures, evaluating their effectiveness and adjusting the instruction based on the evaluations. Comprehensible and structured learning environments this includes strategies such as organising the instructional setting, providing a schedule of activities that is kept up to date, carefully planning and providing choice-making opportunities, providing preventive behavioural support and providing supports to assist with transitions, flexibility and change. It resources for making visual supports, and is important that one person takes responsibility an understanding of and empathy with the for coordinating what is required so that student�s perspective. It is particularly important that students have a lot of support at the beginning of each year to learn the routines and rules, as well as the exceptions. Careful consideration should be given to the functionality of the skills, with an emphasis on skills that: are most likely to be useful for the student to control his or her environment will increase the student�s independence and quality of life will increase the student�s competent performance.
Autosomal dominant nocturnal ing birth control pills 4 periods a year generic discount levonorgestrel 0.18 mg line, and confusional arousals in the general population: their fre frontal lobe epilepsy in a Spanish family with a Ser252Phe mutation quency and relationship to birth control pills gain weight order levonorgestrel american express other sleep and mental disorders birth control for women mostly by barbara discount levonorgestrel on line. Prevalence and genet 1988;297:592 ics of sleepwalking: a population-based twin study birth control pills gain weight buy discount levonorgestrel 0.18 mg. The use of sched 1997;48:177-181 uled awakenings to eliminate childhood sleepwalking. The role of sleep and the activity profile within frontal and parietal cortices: a sleep disorder center in evaluating sleep violence. Nightmares and dissociative possible indicator for alpha-synucleinopathy demonstrated by dopa experiences: the key role of childhood traumatic events. Clinical importance of night 2004;251:781-794 mare disorder in patients with dissociative disorders. A sensorimotor approach to the treatment sleep behavior disorder in neurologic disorders: results in 14 pa of trauma and dissociation. Exploding head syndrome and idiopathic stabbing ior disorder in 33 polysomnographically confirmed cases. Status dissociatus-a perspective on graphic recordings and therapeutic suggestions. Clinical and polysomnographic features of sleep pathologic associations of sleep paralysis in the general population. Catathrenia (nocturnal groan ial aggregation and association with psychiatric disorders in a na ing): a new type of parasomnia. Development of disturbing dreams during adolescence and their relation to anxiety symptoms. Treatment of chronic nightmares in adjudicated adolescent girls in a residential facility. This Guideline document is limited to a number of common clinical pathologies in paediatric urological practice, as covering the entire field of paediatric urology in a single guideline document is unattainable. The majority of urological clinical problems in children are specialised and in many ways differ to those in adults. This publication intends to outline a practical and preliminary approach to paediatric urological conditions. Complex and rare conditions that require special care with experienced doctors should be referred to designated centres where paediatric urology practice has been fully established and a multidisciplinary team is available. Over time, paediatric urology has developed and matured, establishing its diverse body of knowledge and expertise and may now be ready to distinguish itself from its parent specialties. Thus, paediatric urology has recently emerged in many European countries as a distinct subspecialty of both urology and paediatric surgery and presents a unique challenge in the sense that it covers a large area with many different schools of thought and a huge diversity in management. Knowledge gained by increasing experience, new technological advances and non-invasive diagnostic screening modalities has had a profound influence on treatment modalities in paediatric urology, a trend that is likely to continue in the years to come. It must be emphasised that clinical guidelines present the best evidence available to the experts but following guideline recommendations will not necessarily result in the best outcome. Guidelines can never replace clinical expertise when making treatment decisions for individual patients, but rather help to focus decisions also taking personal values and preferences/individual circumstances of children and their caregivers into account. These are abridged versions which may require consultation together with the full text version. A number of translated versions, alongside several scientific publications in European Urology, the Associations scientific journal are also available [1-3]. This 2018 publication includes a number of updated chapters and sections as detailed below. Initially offer urotherapy involving bladder rehabilitation and bowel 2 Weak management. If bladder bowel dysfunction is present, treat bowel dysfunction first, before 2 Weak treating the lower urinary tract condition. Offer supportive measures in conjunction with other treatment modalities, of 1 Strong which pharmacological and alarm treatment are the two most important. Start early anticholinergic medication in the new-borns with suspicion of an 2 Strong overactive detrusor. Treatment should be started with mild laxatives, rectal suppositories as well as digital. The risk of surgical and non-surgical complications and consequences outweigh the risk for permanent damage of the upper urinary tract +/ incontinence due to the detrusor. In patients with a neurogenic bladder and a weak sphincter, a bladder outlet 3 Weak procedure should be offered. A life-long follow-up of renal and reservoir function should be available and 3 Weak offered to every patient. Addressing sexuality and fertility starting before/ during puberty should be offered. Treatment Select treatment based on symptoms, 3 Weak function and reflux as well on surgical and parenteral choices: observation, endoscopic decompression, ureteral re-implantation, partial ephroureterectomy, complete primary reconstruction. Treatment In non-functioning moieties with recurrent 3 Weak infections, heminephro-ureterectomy is a definitive solution. Ureteral reconstruction (ureteral re-implantation/ureteroureterostomy/ ureteropyelostomy and upper-pole ureterectomy) are other therapeutic options, especially in cases in which the upper pole has function worth preserving. Application of a structured analysis of the literature was not possible in many conditions due to a lack of well-designed studies. Clearly there is a need for continuous re-evaluation of the information presented in this document. These key elements are the basis which panels use to define the strength rating of each recommendation. The strength of each recommendation is represented by the words �strong� or �weak� [8]. The incidence of phimosis is 8% in six to seven year olds and just 1% in males aged sixteen to eighteen years [10]. Balanitis xerotica obliterans, also termed lichen sclerosis, has been recently found in 35% circumcised prepuce in children and adolescents and in 17% of boys younger than ten years presenting with phimosis. Phimosis has to be distinguished from normal agglutination of the foreskin to the glans, which is a more or less lasting physiological phenomenon with clearly-visible meatus and free partial retraction [13]. Separation of the prepuce from the glans is based on accumulated epithelial debris and penile erections. Forceful preputial retraction should be discouraged to avoid cicatrix formation [14]. It interferes with perfusion distally from the constrictive ring and brings a risk of preputial necrosis. If the prepuce is not retractable, or only partly retractable, and shows a constrictive ring on drawing back over the glans penis, a disproportion between the width of the foreskin and the diameter of the glans penis has to be assumed. In addition to the constricted foreskin, there may be adhesions between the inner surface of the prepuce and the glanular epithelium and/or a fraenulum breve. Paraphimosis is characterised by a retracted foreskin with the constrictive ring localised at the level of the sulcus, which prevents replacement of the foreskin over the glans. The steroid therapies were more effective over placebo and manual stretching [15]. The hypothalamic pituitary-adrenal axis was not influenced by local corticoid treatment [22]. Operative treatment of phimosis in children is dependent on the caregivers� preferences and can be plastic or radical circumcision after completion of the second year of life. Alternatively, the Shang Ring may be used especially in developing countries [23]. Plastic circumcision has the objective of achieving a wide foreskin circumference with full retractability, while the foreskin is preserved (dorsal incision, partial circumcision, trident preputial plasty) [24]. However, this procedure carries the potential for recurrence of the phimosis [25]. In the same session, adhesions are released and an associated fraenulum breve is corrected by fraenulotomy. Simple ballooning of the foreskin during micturition is not a strict indication for circumcision. A recent meta-analysis could not find any risk in uncircumcised patients without a history of phimosis [31]. Contraindications for circumcision are: an acute local infection and congenital anomalies of the penis, particularly hypospadias or buried penis, as the foreskin may be required for a reconstructive procedure [32, 33].
Assess the child�s physical birth control for women yeezy purchase levonorgestrel 0.18mg with mastercard, emotional birth control mirena buy line levonorgestrel, social birth control pills 45 year old woman order genuine levonorgestrel online, and educational needs and 8431 how these needs may be met if under the care of a guardian birth control pills 40s discount levonorgestrel uk. Consider the appropriateness of the child maintaining a relationship with 8433 parents if reunification efforts are discontinued. If adoption 8435 is ruled out, document compelling or justifiable reasons not to terminate 8436 parental rights and pursue adoption. Determine if guardianship is the next best permanency goal to the 8438 primary goal. Identify prospective guardians who are fit and willing to be ongoing 8440 caregivers for the child, and who will support the safety, permanency, 8441 and well-being of the child. If the prospective guardian is a non-relative, the child 8443 must be currently placed in their home or be a sibling of a child placed in 8444 the home. Discuss with prospective guardians the long-term view for the child and 8446 ability and willingness to be an ongoing caregiver if the current primary 8447 permanency goal is discontinued. Provide full disclosure of requirements and responsibilities of 8449 guardianship to the prospective guardians and child�s parent(s) including 8450 continuation of parental visitation and residual parental rights. Identify factors that must be considered for transition planning if the 8452 concurrent goal becomes the primary goal. The following steps should be completed by the 8455 permanency caseworker during the selection process while choosing guardianship as a 8456 primary goal for a child in foster care: 8457 1. Discuss guardianship as a primary goal in the context of a Child and Family Team 8458 Meeting. If available, include the regional guardianship subsidy caseworker as a 8459 participant in the planning process. Assess the child�s physical, emotional, social, and educational needs and how 8461 these needs may be met if under the care of a guardian, including specific 8462 sources of support such as: 8463 a. Availability of financial support for the child (such as Supplemental 8464 Security Income, Social Security benefits, or other benefits), as well as the 8465 prospective guardian resources, specified relative payment (if a qualifying 8466 relative), or guardianship subsidy for non-relatives; 8467 b. Ability to address health care needs through health care coverage such as 8468 the guardian�s insurance or Medicaid, if the child qualifies; 8469 c. Need for ongoing services from Child and Family Services or the 8470 Department of Human Services. Child�s citizenship and legal residency status, and if an undocumented 8472 alien, how the child�s medical needs can be met without Medicaid 8473 coverage. Identify prospective guardians who are fit and willing to be ongoing 8475 caregivers for the child, and who will support the safety, permanency, 8476 and well-being of the child. If the prospective guardian is a non-relative, the child 8478 must be currently placed in their home or be a sibling of a child placed in 8479 the home. For relative placement, Kinship Practice Guidelines (Section 8480 500) must be followed prior to selecting guardianship as a primary goal. Ensure that the identified licensed caregiver or relative meets the 8482 qualifying factors to become a guardian (see Section C, Guardianship 8483 Qualifying Factors) and that long-term placement with the caregiver or 8484 relative is in the child�s best interest. Obtain commitment of the prospective caregiver to become guardian of 8486 the child and provide for the child�s long-term needs. Discuss the appropriateness of the child maintaining a relationship with 8488 parents despite discontinuation of reunification efforts, including 8489 continuing visitation and residual parental rights. Document that adoption has been ruled out as an appropriate 8491 permanency option for the child and identify compelling or justifiable 8492 reasons not to terminate parental rights and pursue adoption. Provide full disclosure of requirements and responsibilities of 8495 guardianship to the prospective guardian and child�s parent(s). Arrange for an orientation to be provided to the guardian prior to the 8497 transfer of custody. The orientation will include full disclosure of the 8498 benefits and responsibilities of guardianship as well as ensure that they 8499 understand the guardianship agreement. Notify the regional eligibility caseworker of the pending foster care case 8501 closure and if a guardianship subsidy is planned. Have the prospective guardian 8504 complete the form 30 days prior to custody and guardianship 8505 being transferred to the guardian. Select a concurrent goal by identifying the next best permanency goal for 8512 the child. Prepare a transition plan with the Child and Family Team, including 8517 parental visitation, safety planning and identification of community 8518 resources available to support the needs of the child and guardian. Request that the court grant custody and guardianship to the prospective 8522 guardian, when transition planning is complete. Occur prior to the court granting custody and guardianship to the prospective 8526 guardian, preferably in the context of a Child and Family Team Meeting. Will include notification of the legal rights and responsibilities of the guardian. Include an explanation to parents of their responsibility to continue payment for 8532 the child�s care until the child reaches age 18. The Office of Recovery Services 8533 will continue to collect these child support payments until all obligations are 8534 met. Notify the parents that for tax purposes, their child is considered a dependent of 8536 the guardian. Prior to custody and guardianship being granted to the prospective guardian, the 8540 permanency caseworker must provide an orientation to fully disclose the 8541 responsibilities, benefits, and implications of becoming a child�s legal guardian. The orientation and full disclosure will occur in the context of a Child and Family 8544 Team Meeting prior to court. Legal rights and responsibilities of a guardian (see Section A, 8555 Guardianship and Legal Custody); 8556 b. Financial resources (relative and non-relative); 8559 (1) Guardianship subsidy for non-relatives; 8560 (2) Monthly guardianship subsidy payments may be lower than 8561 current foster care payment. Medicaid: 8567 (1) Qualifying criteria; 8568 (2) Application process; 8569 (3) Change in mental health coverage under Medicaid; 8570 (4) Interstate Medicaid eligibility. Adoption after guardianship (non-relative): 218 Utah�s Division of Child and Family Services Out-of-Home Services Practice Guidelines Revised June 2016 8572 (1) Loss of Federal subsidy if guardian later decides to adopt (if child 8573 would have qualified for Federal funding while in care); 8574 (2) No guarantee for adoption assistance (state funded). Provisions of guardianship agreements, renewals and annual re 8576 certifications. Child and Family Services support resources and contact information for 8579 follow-up and changes. Once approved by the regional guardianship subsidy screening 8588 committee, the permanency caseworker will request an Assistant Attorney General to 8589 file a petition with the juvenile court to: 8590 1. Each region will designate a caseworker who will respond to requests for 8596 information, assistance and provide crisis intervention for guardians. Child and Family Services may provide voluntary home-based or youth advocate 8598 services to help maintain the guardianship placement, within available region 8599 resources designated for this purpose. Child and Family Services may work with the Assistant Attorney General to 8601 request a petition for court-ordered services when appropriate. The permanency caseworker is responsible to notify the eligibility caseworker 8605 that guardianship is the child�s permanency plan and the approximate date for 8606 custody to be terminated. This will help ensure that Medicaid coverage can 8607 continue without interruption for an eligible child. The permanency caseworker 8608 will also let the eligibility caseworker know if a guardianship subsidy is planned 8609 for the child. The permanency caseworker will work with the prospective guardian to 8614 complete the review form within 30 days prior to guardianship being granted by 8615 the court. Unearned Income and Guardianship: Unearned income sources must be 8630 considered when determining if a guardianship subsidy is appropriate for a child 8631 and in determining the amount of the subsidy. The most common types of 8632 Federal unearned income received by children in out-of-home care are 8633 Supplemental Security Income and Social Security Dependent Benefits. The Social Security Administration conducts a 8639 review when an individual reaches age 18 to determine if benefits may continue 8640 into adulthood. For example, a child may receive these dependent 8650 benefits as a result of a parent�s disability or death. Social Security benefits will generally 8652 continue for a child when in the care of a guardian and will not be reduced by 8653 other earnings, including a guardianship subsidy.
Order 0.18 mg levonorgestrel otc. How do Birth Control Family Planning methods work? Which Contraceptive is best for me - Hindi.