

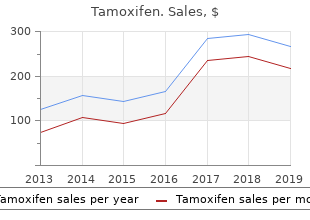
Tamoxifen
"20mg tamoxifen fast delivery, list of women's health issues."
By: Paul Reynolds, PharmD, BCPS
- Critical Care Pharmacy Specialist, University of Colorado Hospital
- Clinical Assistant Professor, Department of Clinical Pharmacy, Skaggs School of Pharmacy and Pharmaceutical Sciences, University of Colorado, Aurora, Colorado

http://www.ucdenver.edu/academics/colleges/pharmacy/Departments/ClinicalPharmacy/DOCPFaculty/Q-Z/Pages/Paul-Reynolds,-PharmD.aspx
When this is achieved it will encourage bundled payment for mothers covered by commercial insurance menstruation 2 weeks after birth safe 20 mg tamoxifen. As a new model that challenges institutional and bureaucratic inertia menstrual exercises purchase tamoxifen with paypal, progress has been slow pregnancy games buy cheap tamoxifen 20 mg online. A frequent response to menstrual insomnia proven tamoxifen 20 mg our efforts has been that the Feds will not allow bundled payment for the perinatal episode. We are very encouraged to find the opposite in our background reading about the purpose of this committee. Although the current perinatal care system focuses on mothers and babies with complications, the majority of pregnant women and babies are low-risk. These factors can exist prior to pregnancy and they 8 can also develop for the mother and/or baby during pregnancy and birth. The percentage of low-risk pregnancies is above 70%, but many of those mothers receive too many intensive obstetrics services, and too few high value supportive services. A list of our Exclusionary Risk Criteria is included in the Supplementary Information Section. Mothers with preexisting complications are referred to physician care, and if a mother or baby develops complications during pregnancy that require care outside the bundled price the clinical care is seamless. A 30 year-old second time mother began care at 10 weeks and received all of her prenatal visits at the birth center. She progressed slowly in labor and had significant unrelieved discomfort with contractions. Per protocol she was non-emergently transferred to the hospital for continuous fetal heart rate monitoring. Six hours after transfer the fetal heart tracing showed persistent decelerations of the fetal heart rate. Sometimes it is difficult to get agreement on what constitutes the bundle of perinatal care services. This includes all professional and facility fees during labor and birth the most expensive time of the episode. In addition, prenatal education, doulas and lactation support services are included in the package of care. This includes Medicare, which pays annually for the care of 15,000 mothers-300 per year in Minnesota. Quality and Cost Our BirthBundle model has the ultimate goal of providing comprehensive perinatal care that maximizes the chances for the mother and baby to have healthy and satisfying outcomes while minimizing the use of unnecessary interventions all for a price that is less than current fee for service amounts. Comparing cesarean section rates is reasonable, but it is important to assess comparable groups of mothers. The most useful rate is assessed in first time mothers (Nulliparas), at 37-42 weeks (Term), with one baby (a Singleton) that is headfirst (Vertex). The recent review in Consumer Reports shows that this rate varies widely around the country and even between hospitals in the same 6 community. Of the 29% who need hospital care, 12% transfer during or after birth and another 17% of mothers are transferred to hospital care prior to labor (for breech presentation or labor <37 or > 42 weeks gestation). This higher percentage of first time mothers increases the workload impact because of the greater amount of time and effort spent by midwives in attending these births. The labors of nulliparous mothers are longer than those of mothers who have had a prior birth, and the need for cesarean section is increased. In summary, cost savings are realized through a lower-intervention model of maternity care that is highly-coordinated and leverages the use of a birth center, a lower-cost facility. Payment Methodology the adage that you get what you pay for is true for medical care. When perinatal care providers are paid for each procedure, each imaging study and each patient encounter they are working in a perverse productivity model. This is a model that is virtually certain to increase the output of procedures, imaging studies and patient visits without generating a product that promotes health or heals disease. We have designed the BirthBundle as a valuable clinical service product imbedded in a new payment model. Some incremental progress has been made recently with the advent of blended facility and professional fees that are the same for vaginal births and cesarean sections. This initial limited perinatal payment innovation led to a decrease in intrapartum costs and possible decreases in C/S rates. The important next step is to widen the scope of the episode, and to implement comprehensive bundled perinatal episode payments. Some initial payer resistance to bundled payment was due to concerns about billing infrastructure that only supported fee for service payments. This is surmountable by continuing to use the fee for service billing infrastructure to construct the bundled payment. Some states have provided retrospective bundled payment for perinatal care identified by attribution models based on who attends the birth of the baby. This is problematic since the person or team attending the birth may have never seen the mother prenatally. We can also build in a reasonable margin to provide sustainability and growth for this model of care. But in Minnesota, as in many other states, historical Medicaid payments are very low and are a major barrier to the implementation of bundled payments. Directing the adequate, already allocated public funds to perinatal providers in the form of bundled payments is much more likely to lead to higher value care. This would include help in determining the appropriate amount of the bundled payment as well as the timing of its distribution. In addition, we would like to explore the possibility of having providers take on additional risk beyond the single bundled payment. Finally, stop loss insurance or risk pools will be needed for the rare expensive outlier perinatal cases. Providers should not have to carry the costs of care for many months after performing the service. A solution would be an upfront partial payment at 20 weeks gestation followed by a final retrospective bundled payment shortly after completion of the episode. Providers could also take on additional risk by taking cost responsibility for some multiple of the agreed upon bundled price. The most effective managed care is that which is closest to the patient and the provider. Large clinical and temporal distances between the payer, the provider and the patient present major problems. The aim of the BirthBundle is not to manage care as much as it is to empower mothers to collaborate in the provision of their care within an improved system. Value over Volume Investment in perinatal care has the longest time frame and the largest return of any type of medical care. The challenge is to maximize the value of the care provided to mothers and babies. Pregnancy ultrasound is a useful tool that has provided many benefits over the three decades since it came into wide use. In a recent national survey 70% of mothers had 3 or more scans, and 23% had more than 7 scans. In addition, many of the scans done late in pregnancy drive inappropriate clinical decisions such as induction of labor for presumed large babies. The savings derived from fewer cesarean sections and lower facility fees for the majority of women would offset the costs associated with the small number of complicated births that would require hospital care. A specific pregnancy insurance component could provide outlier payment adjustments if the costs for a patient or her baby exceeded a certain amount. This would reduce the financial risk to providers and facilities participating in the bundled payment program. Physicians and midwives who provide pregnancy and newborn care all intend to provide the highest quality of care to mothers and babies. Unfortunately, traditional clinical system silos and the fee for service payment system discourage collaboration by paying for pieces of the perinatal care episode provided by disconnected entities. At present, the system focuses on the most complicated and expensive pieces of the episode.
The effects of ischaemia are variable and range Interlobular arteries of the kidneys womens health of blairsville order genuine tamoxifen line. No effects on the tissues menopause exhaustion purchase tamoxifen 20mg otc, if the collateral channels blockage of one vessel can re-establish blood supply develop adequately so that the effect of ischaemia fails to menstrual wheel discount tamoxifen 20mg overnight delivery bypassing the blocked arterial branch menopause mood swings tamoxifen 20 mg without a prescription, and hence the occur. These result when collateral example: channels are able to supply blood during normal activity but Superior mesenteric artery supplying blood to the small the supply is not adequate to withstand the effect of exertion. The examples are angina pectoris and intermittent Inferior mesenteric artery supplying blood to distal colon. The cause of sudden death from ischaemia vi) Blood pigments, haematoidin and haemosiderin, liberated is usually myocardial and cerebral infarction. At this stage, the most important and common outcome of ischaemia most infarcts become pale-grey due to loss of red cells. There are a few other noteworthy Grossly, infarcts of solid organs are usually wedge features in infarction: shaped, the apex pointing towards the occluded artery Most commonly, infarcts are caused by interruption in and the wide base on the surface of the organ. Recent infarcts are generally of coronary arteries may produce myocardial infarction due slightly elevated over the surface while the old infarcts to acute coronary insufficiency. Infarcts are classified depending Microscopically, the pathognomonic cytologic change in upon different features: all infarcts is coagulative (ischaemic) necrosis of the 1. In cerebral infarcts, Pale or anaemic, due to arterial occlusion and are seen in however, there is characteristic liquefactive necrosis. Red or haemorrhagic, seen in soft loose tissues and are At the periphery of an infarct, inflammatory reaction is caused either by pulmonary arterial obstruction. Initially, neutrophils predominate but subsequently lungs) or by arterial or venous occlusion. In cerebral Recent or fresh infarcts, the liquefactive necrosis is followed by gliosis i. Old or healed replacement by microglial cells distended by fatty material (gitter cells). According to presence or absence of infection: Bland, when free of bacterial contamination Septic, when infected. Myocardial infarction (Chapter 16), cerebral infarction ii) Within a few hours, the affected part becomes swollen (Chapter 30) and infarction of the small intestines (Chapter due to oedema and haemorrhage. The amount of haemorrhage 20) are covered in detail later in respective chapters of is variable, being more marked in the lungs and spleen, and Systemic Pathology. Embolism of the pulmonary arteries may tion appear early, while death of the cells. Cut surface is 127 dark purple and may show the blocked vessel near the apex of the infarcted area. Microscopically, the characteristic histologic feature is coagulative necrosis of the alveolar walls. Initially, there is infiltration by neutrophils and intense alveolar capillary congestion, but later their place is taken by haemosiderin, phagocytes and granulation tissue (Fig. Majority of them are caused by thromboemboli, most commonly originating from the heart such as in mural thrombi in the left atrium, myocardial infarction, vegetative endocarditis and from aortic aneurysm. Less commonly, renal infarcts may occur due to advanced renal artery atherosclerosis, arteritis and sickle cell anaemia. Characteristically, they are pale or anaemic and wedge-shaped with base resting under the capsule and apex pointing towards the medulla. Generally, a narrow rim of preserved renal tissue under the capsule is spared because it draws its blood supply from the capsular vessels. Cut surface of renal infarct in the first 2 to 3 days is red and congested but by 4th day the centre becomes pale yellow. At the end of one week, the infarct is typically anaemic and depressed below the surface of the kidney Figure 5. Microscopically, the affected area shows characteristic coagulative necrosis of renal parenchyma i. The margin of the infarct shows inflammatory reaction?initially acute but later Grossly, pulmonary infarcts are classically wedge-shaped macrophages and fibrous tissue predominate (Fig. Spleen is one of the common sites for their base at the periphery and apex pointing towards infarction. Occlusion is caused most Microscopically, the features are similar to those found commonly by thromboemboli arising in the heart. Coagulative necrosis and mural thrombi in the left atrium, vegetative endocarditis, inflammatory reaction are seen. Later, the necrotic tissue myocardial infarction), and less frequently by obstruction of is replaced by shrunken fibrous scar (Fig. Obstruction of the portal vein is usually Grossly, splenic infarcts are often multiple. They are secondary to other diseases such as hepatic cirrhosis, characteristically pale or anaemic and wedge-shaped with intravenous invasion of primary carcinoma of the liver, Figure 5. The affected area shows outlines of cells only due to coagulative necrosis while the margin of infracted Figure 5. Infarcts lower extremity Pale Not lethal carcinoma of the pancreas and pylephlebitis. Infarcts of Zahn portal vein or its branches generally does not produce (non-ischaemic infarcts) produce sharply defined red-blue ischaemic infarction but instead reduced blood supply to area in liver parenchyma. Obstruction of the hepatic artery or its of pale or anaemic infarcts as in kidney or spleen. Infarcts branches, on the other hand, caused by arteritis, of Zahn occurring due to reduced portal blood flow over arteriosclerosis, bland or septic emboli, results in ischaemic a long duration result in chronic atrophy of hepatocytes infarcts of the liver. Inflammation is defined as 2 weeks) and represents the early body reaction, resolves the local response of living mammalian tissues to injury due quickly and is usually followed by healing. It is a body defense reaction in order to eliminate the main features of acute inflammation are: or limit the spread of injurious agent, followed by removal 1. Infective agents like bacteria, viruses and their toxins, Sometimes, the acute inflammatory response may be fungi, parasites. Chronic inflammation is of longer duration and occurs either after the causative agent of acute inflammation persists 3. Physical agents like heat, cold, radiation, mechanical for a long time, or the stimulus is such that it induces chronic trauma. The Roman writer Celsus Alteration in the microvasculature (arterioles, capillaries and in 1st century A. These inflammation as: alterations include: haemodynamic changes and changes in rubor (redness); vascular permeability. The earliest features of inflammatory response result from To these, fifth sign functio laesa (loss of function) was changes in the vascular flow and calibre of small blood later added by Virchow. This nomenclature had its origin in old times but is as under: now we know that burning is only one of the signs of 1. With mild form of injury, the blood flow may be re-established in 3-5 these features, thus, elicit the classical signs of inflam 131 seconds while with more severe injury the vasoconstriction mation?redness, heat, swelling and pain. In and around the inflamed tissue, there other components of the microcirculation like venules and is accumulation of oedema fluid in the interstitial compart capillaries. This change is obvious within half an hour of ment which comes from blood plasma by its escape through injury. Vasodilatation results in increased blood volume in the endothelial wall of peripheral vascular bed. In the initial microvascular bed of the area, which is responsible for stage, the escape of fluid is due to vasodilatation and redness and warmth at the site of acute inflammation. But subsequently, the characteristic hydrostatic pressure resulting in transudation of fluid into inflammatory oedema, exudate, appears by increased the extracellular space. Stasis or slowing is followed by leucocytic margination the fluid balance is maintained by two opposing sets of forces: or peripheral orientation of leucocytes (mainly neutrophils) along the vascular endothelium. The leucocytes stick to the i) Forces that cause outward movement of fluid from vascular endothelium briefly, and then move and migrate microcirculation are intravascular hydrostatic pressure and through the gaps between the endothelial cells into the colloid osmotic pressure of interstitial fluid. This process is known as emigration ii) Forces that cause inward movement of interstitial fluid (discussed later in detail). Lewis Whatever little fluid is left in the interstitial compartment induced the changes in the skin of inner aspect of forearm is drained away by lymphatics and, thus, no oedema results by firm stroking with a blunt point.
Order tamoxifen 20 mg without prescription. I MET MC LYTE! Dallas Ultimate Women’s Expo VLOG.
Rarely menstrual 30 day cycle cheap tamoxifen 20 mg online, a brain and spinal cord pregnancy gingivitis best buy for tamoxifen, particularly encountered in meningioma may display features of anaplasia and invade carcinomas of the lung and breast menstrual cycle hormones order 20 mg tamoxifen with mastercard. This pattern of Histologically breast cancer pictorial purchase tamoxifen online now, metastatic tumours in the brain meningioma is associated with extraneural metastases, recapitulate the appearance of the primary tumour of mainly to the lungs. Grossly, the metastatic surrounded by an outer layer of fibrous tissue, the epineurium. A less frequent pattern is carcinomatous Each fascicle is composed of bundles of connective tissue, meningitis or meningeal carcinomatosis in which there is the endoneurium. There are 2 main types of nerve fibres or presence of carcinomatous nodules on the surface of the axons comprising a peripheral nerve?myelinated and non myelinated. Nodes of Ranvier on myeli nated fibres are the boundaries between each Schwann cell surrounding the fibre (Fig. Myelinated axons have their origin from neurons in the posterior root ganglia and the anterior horn cell of the spinal cord, whereas non myelinated axons arise from neurons in the posterior root ganglia and in the autonomic ganglia. They are commonly multiple, well-defined and usually located at the grey and capacity as has been discussed on page 172. Normally, the injured axon of Wallerian degeneration, axonal degeneration and segmental a peripheral nerve regenerates at the rate of approximately demyelination (Fig. Wallerian degeneration hampered due to an interposed haematoma or fibrous scar, occurs after transection of the axon which may be as a result the axonal sprouts together with Schwann cells and of knife wounds, compression, traction and ischaemia. It may be polyneuropathy, ration occurs by sprouting of axons and proliferation of mononeuropathy multiplex, and mononeuropathy. In axonal degeneration, noticeable sensory features such as tingling, pricking, degeneration of the axon begins at the peripheral terminal burning sensation or dysaesthesia in feet and toes. The features in the form of muscle weakness and loss of tendon cell body often undergoes chromatolysis. Involvement of the autonomic cell proliferation in the region of axonal degeneration. Most cases have origin loss of axonal integrity occurs, probably as a result of some in acquired metabolic and toxic causes such as thiamine primary metabolic disturbance within the axon itself. Segmental demyelination is loss of myelin of the segment Pathologically, polyneuropathy may be the result of between two consecutive nodes of Ranvier, leaving a axonal degeneration (axonopathy) or segmental denuded axon segment. In each Schwann cell proliferation generally accompanies demyeli type, acute, subacute and chronic forms are distinguished. Guillain-Barre syndrome is the classical example of acute Repeated episodes of demyelination and remyelination are demyelinating polyneuropathy which has probably an associated with concentric proliferation of Schwann cells autoimmune etiology. Mononeuropathy multiplex or multifocal neuropathy Microscopically, the tumour is composed of fibrocellular is defined as simultaneous or sequential multifocal bundles forming whorled pattern. The and compact cellularity (Antoni A pattern) alternating with involvement may be partial or complete and may evolve over loose acellular areas (Antoni B pattern). Multifocal neuropathy represents part of pattern show palisaded nuclei called Verocay bodies spectrum of chronic acquired demyelinating neuropathy. Nerve fibres are usually found stretched over Mononeuropathy, on the other hand, is focal involve the capsule but not within the tumour. It is generally the result of local causes degeneration contain haemosiderin and lipid-laden such as direct trauma, compression and entrapment. Tumours of the peripheral nerves are commonly benign and include schwannoma (neurilemmoma) and neurofibroma. Intraspinal schwannomas are found Neurofibromatosis type 1 is a genetic disorder having as intradural tumours in the thoracic region. In the peripheral mutation in chromosome 17 while type 2 has mutation in nerves, they occur as solitary nodule on any sheathed chromosome 22. Neurofibromatosis may involve a 894 Neurofibromas have tendency for local recurrences after excision. Neurilemmoma virtually never turns malignant, while sarcomatous transformation in neuro fibroma, particularly in neurofibromatosis, is not unusual. The contrasting features to distinguish neurofibroma from schwannoma are listed in Table 30. The tumour may arise de novo or from malignant transformation of a pre-existing neurofibroma than a schwannoma, generally at an early age (20-40 years). The main mass is multilobulated with increased fat while lower part of the image shows a with neurofibromatosis type 1 with chromosomal deletion separate encapsulated gelatinous mass. Cut surface of both the masses 17p and p53 gene mutations, while some develop at sites of shows circumscribed, gelatinous, lobulated grey-white firm masses. Grossly, the tumour group of nerves or may occur as multiple, oval and appears as an unencapsulated fusiform enlargement of a irregular swellings along the length of a nerve (plexiform neurofibroma) (Fig. Microscopically, a neurofibroma is composed of bundles Microscopically, the tumour has the general appearance and interlacing fascicles of delicate and elongated spindle of tumour cells resembling a fibrosarcoma. The cells have wavy nuclei and a residual nerve fibre (neurite) is also identified. Location Cerebellopontine angle (vestibular branch of Dermis; along the nerve trunk 8th nerve); extradural sites 2. Genetics Bilateral in association with type 2 neuro Multiple associated with type 1 neuro fibromatosis having autosomal dominant fibromatosis having autosomal dominant inheritance (chromosome 22 disorder) inheritance (chromosome 17 disorder) 4. Gross appearance Firm, encapsulated, Soft, well demarcated but unencapsulated, c/s tan, translucent c/s mucoid, translucent 5. Microscopy Compact areas (Antoni A) and myxomatous Dense collagen fibres and abundant areas (Antoni B), palisading tumour cells extracellular mucoid material (Verocay bodies) 6. Infiltration Encapsulated along the edge of May infiltrate the peripheral nerve nerve without invading it 7. Measurements have been foregoing chapters, normal figures are given alongside the given as width? An alphabetic normal structure of each organ/system that precedes the order has been followed. Pituitary gland (Hypophysis): Secondly, laboratory values may vary with the method Weight 500 mg and mode of standardisation used; reference ranges given Placenta: below are based on the generally accepted values by the Weight at term 400?600 gm standard methods in laboratory medicine. In this section, laboratory values are given in both Testis and epididymis: conventional and international units. The laboratory values given here are divided into three Prefix Prefix Symbol Factor Units of Lengthsections: clinical chemistry of blood (Table A-3), other bodyUnits of Weight Units of Volume 3 fluids (Table A-4), and haematologic values (Table A-5). In kilo k 10 kilometre (km) kilogram (kg) kilolitre (kl) general, an alphabetic order has been followed. Edinburgh, of several authors listed below have been consulted which are gratefully Churchill Livingstone, 1992. Edinburgh, Churchill general references used as the resource material for the book have Livingstone, 1997. Levine B: Eating oneself and uninvited guests: autophagy-related Stevens A, Lowe J: Pathology, 1st ed. Majno G, Joris I: Apoptosis, oncosis and necrosis: an overview of cell Martin P: Wound healing?aiming for perfect skin regeneration. Rappouli R: From Pasteur to genomics: progress and challenges in Davidson A, Diamond B: Autoimmune diseases. N Engl J Ahr A et al: Identification of high risk breast cancer patients by gene Med 349:583, 2003. Philadelphia, Gray W: Diagnostic Cytopathology, Edinburgh, Churchill Livingstone, 1995. London, Guilherme L, Kalil J: Rheumatic fever: from sore throat to autoimmune Churchill Livingstone, pp 167, 1997. N Engl J Brandtzaeg P et al: Immunopathology of human inflammatory bowel Med 345: 1318, 2001. MacGowan et al: Helicobacter pylori and gastric acid, biological and Angiology 52: 89, 2001. Curr Opin Pul Med 3: examination and staging and determination of prognostic factors. Baker P, Esther O: A practical approach to intraoperative consultation in gynaecologic pathology. As new services become available, demand increases and procedures that give maximum health gain must be prioritised. If the provider does not comply with the terms of any Prior Approval Scheme in providing a service, the commissioners will not be liable to pay for that service. Compliance with this policy will be monitored via regular benchmarking reports and case note audits. To support this approach a set of Core Clinical Eligibility Criteria have been developed and are set out below; patients may be referred in accordance with the referral process if they meet these criteria.
Review of electronic fetal monitoring women's health center flint mi cheap 20 mg tamoxifen visa, including maternal?fetal out comes breast cancer facts cheap tamoxifen 20 mg mastercard, toward a goal of standardizing nomenclature and patient care mensural notation buy tamoxifen 20 mg free shipping. Review of perinatal statistics menopause the musical chicago cost of tamoxifen, the pathology related to all deaths, and significant surgical specimens. Review of patient satisfaction data, complaints, and compliments Perinatal Outreach Education Design and coordination of a program for perinatal outreach education should be provided jointly by neonatal and obstetric physicians and advanced practice registered nurses. Responsibilities should include assessing educational needs; planning curricula; teaching, implementing, and evaluating the program; col lecting and using perinatal data; providing patient follow-up information to referring community personnel; writing reports; and maintaining informative working relationships with community personnel and outreach team members. Ideally, a maternal?fetal medicine specialist, a certified nurse?midwife or certified midwife, an obstetric nurse, a neonatologist, and a neonatal nurse should be members of the perinatal outreach education team. Other profes sionals (eg, a social worker, respiratory therapist, occupational and physical therapist, or nutritionist) also may be assigned to the team. Each member should be responsible for teaching, consulting with community professionals as needed, and maintaining communication with the program coordinator and other team members. Each subspecialty care center in a regionalized or integrated system may organize an education program that is tailored to meet the needs of the peri natal health professionals and institutions within the network. The various educational strategies that have been found to be effective include seminars, audiovisual and media programs, self-instruction booklets, and clinical practice rotations. Perinatal outreach education meetings should be held at a routine time and place to promote standardization and continuity of communication among community professionals and regional center personnel. As mandated by the subspecialty boards and the Accreditation Council for Graduate Medical Inpatient Perinatal Care ServicesCare of the Newborn 3737 Education, a facility providing subspecialty care that has a fellowship training program must have an active research program. Support also should be available for at least one ongoing, active quality improvement initiative (see also Chapter 3, Quality Improvement and Patient Safety). Physical Facilities the physical facilities in which perinatal care is provided should be conducive to care that meets the unique physiologic and psychosocial needs of newborns and their families (see also Patient-Centered and Family-Centered Health Care in Chapter 1). Special facilities should be available when deviations from the norm require uninterrupted physiologic, biochemical, and clinical observa tion of patients throughout the perinatal period. Labor, delivery, and newborn care facilities should be located in proximity to each other. When these facilities are distant from each other, provisions should be made for appropriate transi tional areas. The following recommendations are intended as general guidelines and should be interpreted with consideration given to local needs. Individual limi tations of physical facilities for perinatal care may impede strict adherence to these recommendations. Provisions for individual units should be consistent with a regionalized perinatal care system and state and local public health regu lations. The service should be consolidated in a designated area that is physically arranged to prohibit unre lated traffic through the service units. The obstetric facility should incorporate the following components of maternity and newborn care. Fetal diagnostic testing (eg, nonstress and contraction stress testing, biophysical profile, amniocentesis, and ultrasound examinations) 38 Guidelines for Perinatal Care. Labor observation and evaluation for patients who are not yet in active labor or who must be observed to determine whether labor has actually begun; hospital obstetric services should develop a casual, comfortable area (?false-labor lounge) for patients in prodromal labor. Postpartum maternal and newborn care Where rooms are suitably sized, located, and equipped, some or all of the components of maternity care listed previously can be combined in one or more rooms. Combining functions into labor, delivery, and recovery rooms maximize economy and flexibility of staff and space. The traditional obstetric program model?with separate rooms for labor, delivery, recovery, and postpartum care?has become obsolete in new construction guidelines, such as the 2010 Guidelines for Design and Construction of Health Care Facilities. The following facilities should be available to both the antepartum unit and the postpartum unit and, in appropriate circumstances, may be shared. Medical records area with a flat writing surface, computers with access to electronic medical records, or both. Sibling visiting area Inpatient Perinatal Care ServicesCare of the Newborn 3939 the need for care of extremely obese patients is growing for all medical and surgical units in the United States, including maternity units. These patients require more space for antenatal, intrapartum, and postpartum care; staff; and equipment able to support heavier weights. The obstetric department, in conjunction with the hospital administration, should establish written policies according to state and local regulations indicating which nonobstetric patients may be admitted to the labor and delivery suite. Under all circumstances, however, labor and delivery patients must take precedence over nonobstetric patients in this area. Clean gynecologic operations may be performed in the delivery rooms if patients are adequately screened to eliminate infectious cases and if enough personnel are present to prevent any compromise in the quality of obstetric care. Combined Units Comprehensive obstetric and neonatal care is optimally provided for women at both low risk and high risk and their healthy newborns in a labor, delivery, and recovery unit that uses another room for mother?baby postpartum care. Alternatively, care can be provided in a conventional obstetric unit that uses dif ferent rooms for labor, delivery, recovery, and newborn care. Registered nurses who are cross-trained in antepartum care, labor and delivery care, postpartum care, and neonatal care should staff this unit, increasing the continuity and quality of care. Each labor, delivery, and recovery room is a single-patient room containing a toilet and shower with optional bathtub. A sink should be located in each room for scrubbing, handwashing, and neonate bathing. A window with an outside view is desirable in the labor, delivery, and recovery room. Each room should contain a birthing bed that is comfortable during labor and can be read ily converted to a delivery bed and transported to the cesarean delivery room when necessary. Separate oxygen, air, and suction facilities for the woman and the neonate should be provided in two separate locations. Gas outlets and wall-mounted equipment should be easily accessible but may be covered with a panel. Either a ceiling 40 Guidelines for Perinatal Care mount or a portable delivery light may be used, depending on the preference of the obstetric staff. Proper care of the woman in labor requires sufficient space for a sphyg momanometer, stethoscope, fetal monitor, infusion pump, regional anesthesia administration, and resuscitation equipment at the head of the bed. The family area should be farthest from the entry to the room, and there should be a comfortable area for the support person. Equipment needed for labor, delivery, newborn resuscitation, and newborn care should be stored either in the room or in a nearby central storage or supply area and should be immediately available to the labor, delivery, and recovery room. For ease of movement, space below the foot of the bed should be ade quate to accommodate staff and equipment brought into the room. Standard major equipment held in this area for delivery should include a fetal moni tor, delivery case cart, linen hamper, and portable examination lights. A unit equipped for neonatal stabilization and resuscitation (described in Neonatal Functional Units later in this chapter) should be available during delivery. The workable size of a labor, delivery, and recovery room measures 340 net ft2 (31. This room should be able to accommodate six to eight people comfortably during the childbirth process. Each labor, delivery, and recovery room should have the following equipment and supplies necessary for women in labor. Warming cabinets for solutions and blankets Inpatient Perinatal Care ServicesCare of the Newborn 4141. Adjustable lighting that is pleasant for the patient and adequate for examinations. A writing surface for medical records, computer hookup for medical record purposes, or both. Storage facilities for supplies and equipment There should be adequate space for support persons, personnel, and equipment, and room for the patient to ambulate in labor. Design or renovation should include planning for bedside and workstation information management sys tems and for computer management of medical information. Patients with significant medical or obstetric complications should be cared for in a labor, delivery, and recovery room that is specially equipped with car diopulmonary resuscitation equipment and other monitoring equipment neces sary for observation and special care. Rooms used for intensive care of patients at high risk in hospitals with no designated high-risk units are best located in the labor and delivery area and should meet the physical standards of any other intensive care room in the hospital, with a minimum of 200 net ft2 (18. When patients with significant medical or obstetric complications receive care in the labor and delivery area, the capabilities of the unit should be identical to those of an intensive care unit.