

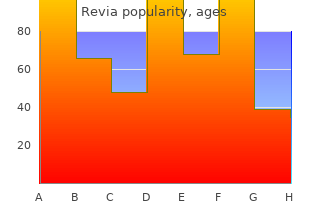
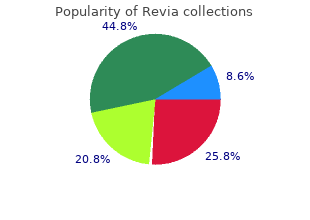
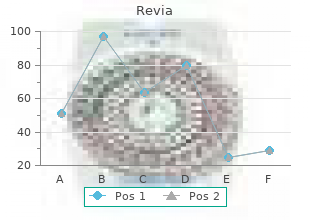
Revia
"Discount 50mg revia otc, medicine in motion."
By: Randolph E. Regal, BS, PharmD
- Clinical Associate Professor, Department of Clinical Pharmacy, College of Pharmacy, University of Michigan
- Clinical Pharmacist, University of Michigan Health System, Ann Arbor, Michigan

https://pharmacy.umich.edu/people/reregal
Therefore symptoms 6 days after embryo transfer discount revia online, in the absence of any conclusive data symptoms narcolepsy 50mg revia sale, the expert opinions expressed in Annex M treatment quad strain buy discount revia on-line, Public Health Measures will assist jurisdictions with the consistent implementation of timely measures that are in line with the objectives of each pandemic period medicine 79 revia 50mg low price, i. The P/T and local planners are encouraged to explore the feasibility and implications of these types of control measures in their jurisdictions and to educate stakeholders. Pandemic infuenza communications planning is based on a strategic risk communications approach. This approach focuses on developing communications that are based on a solid understanding of what people know about pandemic infuenza, what they do not know, and what they want and need to know. Citizens need to be engaged in a dialogue about pandemic infuenza preparedness activities for several reasons: fi Citizens need to be aware of the planning and the preparedness activities so that they are better prepared to take action when they are asked. As the pandemic evolves, the number of organizations that become involved with the media on this issue will be enormous; there will be fnancial issues, human resource issues and social issues�issues that affect every facet of society. Because of the broad scope of these issues, working towards the development of consistent, coordinated messages that various levels of government and stakeholders agree to in advance of a pandemic is critical to ensure that Canadians are prepared to take action to protect themselves and their loved ones. The information demands during a pandemic will be sustained over a long period, resulting in tremendous information demands. Sustaining public confdence over many months will be a huge challenge that will require consistent and coherent messages. All key stakeholders (external, internal, international) must receive consistent and relevant information in a timely manner during any type of emergency. Planning activities are to ensure Preparedness 19 consistent and coherent messaging across Canada as well as predefning roles and responsibilities as much as possible. The objectives of communication planning are to: fi Create a strong communications network (nationally and internationally). The P/Ts produce materials to promote immunization each fall; these are specifc to the programs they offer in their jurisdictions. Most communication materials and strategies, which target the general public, media, health care workers and other community organizations (considered as �external� key stakeholders), are geared to promoting immunization and reducing unnecessary hospital visits. These materials are developed at the P/T and local levels with minimal federal input. To date, there has not been a centrally coordinated education campaign with regard to pandemic infuenza that targets the external key stakeholders. Although campaigns have not been centrally coordinated, substantial work is going into ensuring a greater coordination of key messages. Within the pandemic communications planning process, F/P/T and non-governmental organizations are working on the development of messages that can be adapted to the specifc stakeholders in each jurisdiction. In addition, communications have established several communications networks for F/P/T interaction. Other communication issues are also being addressed as part of the �all hazards approach� to crisis communications. This must be built into our ongoing work plan for pandemic infuenza communications. Communication plans must recognize expertise in the full set of relevant disciplines, as well as accommodate stakeholder knowledge. The strategic risk communications process is the primary means for addressing these integrated communication needs and demonstrating that the risk management process has addressed them. Stakeholders have varying roles and responsibilities; therefore, coordination is crucial to ensure that messages are accurate and consistent and that jurisdictional boundaries are respected. The development of a strategic risk communications plan is underway and would become a key part of communications planning for pandemic infuenza. During the Interpandemic Period, activities will focus on prevention and preparedness. Implementation of the response activities will occur in concordance with each change in Canadian Pandemic Phase. Front-end investment of resources in prevention and preparedness activities will facilitate effective management of the pandemic and mitigation of negative outcomes. To manage an emergency effectively, it is essential to have comprehensive response plans in place. With respect to pandemic planning, the existence of these plans needs to be communicated to all potential stakeholders. Copies should be distributed to organizations and individuals that will be involved in the pandemic response and, if possible, advance testing of these plans should be coordinated with a mechanism to provide feedback for improvement and updating. In Annex A, Planning Checklists, planning activities are listed and grouped according to Plan components. The checklists are designed to facilitate planning at the P/T and local levels, and they essentially refect planning activities that should be undertaken during the Interpandemic Period. The tables include the key actions necessary to facilitate a comprehensive and consistent response to pandemic alerts and an infuenza pandemic. However, it is recognized that additional details and modifcations will need to be added as the pandemic unfolds. For example, it cannot be determined in advance of the appearance of a novel virus when an effective vaccine might be available; therefore, all activities listed under �Vaccine Programs� in the tables may occur at different phases than the ones that are currently listed (in the tables). Therefore if there is concurrent circulation of two or more novel infuenza viruses, the phase will correspond to the situation presenting the highest risk of pandemic. The new terminology includes six phases spanning three pandemic periods: Interpandemic Period, Pandemic Alert Period and the Pandemic Period. A Post-Pandemic Period has also been identifed but it is not linked to a numerical phase. This Response Section has been updated since it was frst published in February 2004 to include this terminology. For responders at the time of a pandemic, the focus will be on more localized �triggers� that may or may not correspond to the Canadian pandemic phase because the phase is based on the highest level of novel infuenza activity observed in Canada. It is expected that differences in infuenza activity within Canada will be described on the basis of surveillance data that is reported similarly to that during the annual infuenza season. Planners at all levels in the health and emergency service sectors, from municipal to federal, are encouraged to think about the �phase� under which their specifc jurisdictions would fall based on infuenza activity within the jurisdictions. This is so they can operationalize an appropriate response for the jurisdiction, recognizing that their plans will also be affected by the epidemiology of the pandemic nationally and globally. The Plan assumes that progression to a pandemic will occur if novel infuenza activity occurring Response 3 during the Pandemic Alert Period is not halted. Therefore the response to novel virus activity during the Pandemic Alert Period may need to be signifcantly modifed from what is outlined in this Plan if the epidemiology. This structure, which indicates roles and responsibilities of specifc groups in response to an emergency, is included in Annex L, Federal Emergency Preparedness and Response System. The specifc composition, roles and responsibilities of the Advance Planning Group still need to be determined; however, members that can provide technical advice specifc to pandemic infuenza will be essential. Also included in Annex L is a fow diagram that aligns response activities with the phases. It is an example of a specifc, technical emergency plan that has been developed as part of much larger initiative to create plans to deal with all types of national emergencies. They recognized that many of the response issues would be the same but on a much larger scale. The response to pandemic infuenza also would need to be sustained for a longer period of time and would likely include a mass immunization effort on top of the demands of acute care for patients. In particular, the need for resources and surge capacity within the health system to deal with public health emergencies is highlighted. In addition, there may be opportunities for reassortment between animal and human infuenza viruses when they simultaneously infect the same swine or human host. Such reassortment events may result in the development of a new infuenza virus subtype with pandemic potential. Since 2003, an unprecedented number of avian outbreaks of infuenza have been detected worldwide. Human cases, ranging in severity from conjunctivitis to fatal cases, have resulted from these various outbreaks. Because the actions in the guideline document pertain to the new Canadian Phases 1. Although the control of animal infuenza outbreaks is a key part of preventing the emergence of a human infuenza pandemic�and there are critical animal and human health linkages�the responses to the actual animal outbreaks are best addressed in animal health guidelines and plans.
Tese meth- the diagnosis of blood and tissue parasitic infections based on ods are also commonly used in smaller laboratories or during published recommendations [288�290] medicine you can order online order generic revia canada. Balamuthia cephalitis due primarily mandrillaris does not grow on standard agar (requires specialized to medicine and technology revia 50 mg sale Naegleria fowleri symptoms toxic shock syndrome generic 50mg revia, cell culture) treatment 1st degree burn buy revia with visa. Stained and unstained tissue slides Balamuthia mandrillaris may also be sent for identifcation of amebic trophozoites and/ (free-living amebae) or cysts. Serology does not distinguish be- Babesia duncani, and tween acute and past infection. Cross- Encysted larvae and/or hooklets can be seen in tissue biopsies or echinococcosis reactivity may be observed between tests for aspirates of cysts (echinococcosis). Filariasis due to species of Microscopy of Giemsa-stained thick and thin blood Blood flms for W. Examination of concentrated blood speci- between 10 am and 2 pm when microflariae are circulating. Mansonella mens (Knott, Nuclepore fltered blood, or buffy coat) Repeat exams may be necessary due to low parasitemia. Antibody and/or antigen de- Serology does not differentiate between these flariae. Histopathologic examina- tion of skin biopsy or resected nodule (onchocercoma) can iden- tify microflariae and/or adults. Calculation of percentage parasitemia (using thick or Plasmodium knowlesi tory blood flms within 12�24 h thin blood flms) is required for determining patient manage- ment and following response to therapy. IgG avidity test and serial titers may distinguish between recent and past infection. Trypanosomiasis, African Microscopy of Giemsa-stained thick and thin blood Plasma cells with large eosinophilic antibody globules may be seen (African sleeping sickness) flms or buffy coat preps. Card agglutination test for trypanosomi- due to Trypanosoma brucei low, requiring repeated exams. American trypanosomiasis Microscopy of Giemsa-stained thick and thin blood Parasitemia is very low in chronic infection. Subsequent sections A and B provide more detailed a small number of infections occurring in California and information on the diagnosis of parasitic infections that are of Washington have been attributed to Babesia duncani, while particular concern to practitioners in North America (babesiosis B. The simian parasite Plasmodium knowlesi has also resources, and expertise of the laboratory performing the tests. Table 73 summarizes the labora- more likely than community laboratories to have the experience tory tests available for these agents. Direct communication by phone or email will sometimes babesiosis is microscopic examination of Giemsa-stained thick hasten specimen processing and result reporting from public and thin blood flms [293, 294]. Although this method requires health laboratories, especially when there is an urgent clinical a minimum amount of resources (staining materials and situation. The availability facilities to have ready access to rapid accurate laboratory test- of rapid shipping methods (FedEx, United Parcel Service, United ing [293]. It is useful to obtain shipping information from such allow rapid detection of the presence of parasites consistent laboratories to avoid unnecessary delays because of customs or with either Plasmodium or Babesia but may not allow for dif- airline regulations or other delivery problems. The thick flm is made using 2�3 drops of blood that have been �laked� (lysed) by placement A. This releases the intracel- Babesiosis is caused primarily by Babesia microti in the United lular parasites and allows for examination of multiple (20�30) States and Babesia divergens in Europe [293]. Use of the �scratch� method will improve adherence and allow for examination as soon as the blood is visibly dry. Store serum refrigerated or frozen if not tested within 4�6 h to preserve antibody and prevent bacterial growth. This test detects fuorescently stained parasites within blood is visibly dry) [294]. It acquires maxi- are prepared like a hematology peripheral smear and are fxed mum efciency for the laboratory if multiple specimens are in ethanol before staining. In addition, it requires preparation of a thin phology for Plasmodium spp identifcation. Wright-Giemsa and rapid method for diagnosis of malaria, it requires considerable time and Field stains are also acceptable. Tere are a number of commercially tion of microflariae, followed by examination under oil immer- available options, although the BinaxNow Malaria is currently sion [290, 291, 293, 294]. Additional felds (at least 300) should be examined for are somewhat less sensitive than thick blood flms and may be patients without previous Plasmodium exposure since they may falsely negative in cases with very low rates of parasitemia and be symptomatic at lower parasite levels [294]. Blood flm examination is also necessary for positive cases expertise for species identifcation, then a preliminary diagno- to confrm the species present and calculate the degree of para- sis of �Plasmodium or Babesia parasites� should be made, fol- sitemia [295]. While munity laboratories) or when the clinical situation is critical and awaiting confrmatory testing, the primary laboratory should an immediate diagnosis is required (stat laboratory in the emer- relay the message to the clinical team that the deadly parasite gency department). Repeat as possible by good-quality thick and thin blood flm examina- blood samples (fi3 specimens drawn 12�24 hours apart, ideally tion. Terefore, the assay should not be used to When Plasmodium spp are identifed, one can enumerate follow patients afer adequate therapy has been given. This is malaria, since antibodies may not appear early in infection and best determined by using the thin flm. Quantifcation can also titers may be too low to determine the status of infection. Serologic turnaround time will be too long to enable rapid institution of testing is also used for blood donor screening. IgG titers of 1:64�1:512 with negative IgM and no titer rises in serial specimens suggest previous infection or B. On stained preparations, the motile trypomasti- in cases empirically treated without prior laboratory diagnosis gote forms typically adopt a �C� shape and can be differentiated by detection of remnant nucleic acid. Of course, these infections can also be likely dif- positive for Plasmodium or Babesia parasites, blood flms must ferentiated on epidemiologic grounds. Motile organisms can also still be examined to determine the percentage parasitemia. Buffy coat concentrate from anticoag- ulated venous blood (thin smear or fresh wet prep for motile organisms) Microscopic examination of tissue aspi- Fluid from needle aspirate of enlarged Fresh aspirated fuid should be stained and examined as 2 h�3 d rates/biopsies by Giemsa/H&E stains lymph nodes or tissue biopsies from soon as possible, preferably within 1 h of sampling. Serum or plasma should be separated from blood within 1 d Plasma is also acceptable for the several hours. She The diagnosis in these stages may be established serologically has received payment for lectures/speakers� bureaus from the New York City or by microscopic examination of tissue aspirates or biopsies. For imens must be handled with care using �standard precautions� activities outside the submitted work, J. He has also received pay- ment for his consultancies to Jewish Hospital (Louisville, Kentucky) and Floyd stages of disease when parasites are no longer easily detected in Memorial Hospital (New Albany, Indiana) and royalties from Taylor Francis, peripheral blood preparations by microscopy. She and her institution have patents and receive mitted by transfusion and transplantation. We acknowledge the contributions and leader- and for her role as Editor of The Journal of Clinical Microbiology. All activities ship provided by Dr Ellen Jo Baron in the 2013 version of this document. Participants included Jennifer Dien Bard, for lectures/speakers� bureaus and travel/accommodations. For activities Christopher Doern, James Dunn, Karen Sue Kehl, Amy Leber, Alex outside the submitted work, S. We especially appreciate the careful review and suggestions of mem- of the manuscript have been disclosed. His institution has ing do not increase recovery of clinically significant microorganisms from stan- received payment for his consultancies with Pfzer and has received grants/ dard automated blood cultures. For activities outside the submitted work, for isolation ofHaemophilus,Actinobacillus,Cardiobacterium,Eikenella, andKingella S. Role of volume of blood cul- She has also received payment for travel/accommodations from the College tured in detection of disseminated infection with Mycobacterium avium com- of American Pathologists, the Clinical and Laboratory Standards Institute, plex [abstract 368]. Detection of bloodstream infections in Consulting and Diagnostic Microbiology Development Program for consul- adults: how many blood cultures are neededfi Blood culture contamination: a ran- American Association of Clinical Chemistry, Hospital and Healthcare System domized trial evaluating the comparative effectiveness of 3 skin antiseptic inter- Association of Pennsylvania, Eastern Pennsylvania Branch of the American ventions. Chlorhexidine versus tincture of iodine for reduc- Society for Microbiology, and Illinois Society for Microbiology for lecture tion of blood culture contamination rates: a prospective randomized crossover honoraria.
The bogeyman has no specific appearance treatment 5th finger fracture revia 50mg sale, and conceptions about him can vary drastically from household to medications definitions order revia american express household within the same community medicine vial caps discount revia 50 mg with mastercard. In many cases treatment meaning buy revia paypal, he has no set appearance in the mind of an adult or child, but is simply a non-specific embodiment of terror. Parents may tell their children that if they misbehave, the bogeyman will get them. Bogeymen may target a specific mischief�for instance, a bogeyman that punishes children who suck their thumbs�or general misbehavior. In many countries, a fictitious scary man similar to a bogeyman is portrayed as a man with a sack on his back who carries naughty children away. This is true for many Latin countries and Eastern Europe, as well as Haiti and some countries in the Far East. In Spain, el hombre del saco is usually depicted as an impossibly ugly and skinny old man who eats the misbehaving children he collects. In Argentina, Chile and particularly in the Southern and Austral Zones, he is mostly known as "El Viejo del Saco" ("The old man with the bag") who walks around the neighbourhood every day around supper time. Googling for �behaviour� produces over 100 million hits, whereas �behaviours� produces 11 million. The expression in paragraph 2, �the brains of these aphasic patients� is different: there, it is specific (to those individual patients). There is a strong of a further reduction in interest rates. It is whether the measures will be successful in practice. It is more than that growth will be slower than the government forecast. Seven out of ten of these cases could not be helped by surgery and more than half will be dead within six months of their diagnosis. The study found that men were more likely to have non-small cell lung cancer, which is less damaging to the lung, and nearly half could be considered operable. Write them here: 78 Grammar for Academic Writing: Unit 7 � Speculating: Conditionals and modals Task 7. The specialists quoted use language that makes it clear that the reasons they give are speculative. Underline the words and phrases that express uncertainty: �Our research suggests women have less resistance to the most dangerous kinds of lung cancer,� he said. Did you underline any expressions which you would not expect to be used in academic writingfi Modal verbs One of the most useful resources for expressing varying degrees of certainty in English is the system of modal verbs. The modals that are usually used in this way are: might would could may should will must Task 7. Another very common use is to speculate about hypothetical situations, often using conditional sentences to do this. For example, you can use a different modal verb in the main clause to indicate more uncertainty: If the findings are inconsistent, we may need to do more experiments. One way to do this is by expressing the idea of the conditional clause as a noun-phrase. This example is from a newspaper report ii: Plans to reduce the legal blood alcohol limit from 80mg to 50mg are to be abandoned by the Government to allow police to concentrate on persistent drivers who ignore the present limit. Government sources confirmed last night that a 10-month investigation into drink-drive reform has produced figures that show a move to lower the limit would save between 30 and 80 lives a year. Underline the three expressions used to show that the information is speculative: It may be that belief in a common truth was far more widespread than the surviving written sources suggest. At about the same time, Nicetas of Byzantium was prompted to counter the opinion that Muslims worshipped the true God, and, early in the next century, the patriarch Nicolas wrote to the caliph that �we have obtained the gift of our authorities [i. This idea never seems to have taken root in Western Europe, and had disappeared completely by the First Crusade. I expect they have received my message by now (because I know how long it normally takes). This time they can be listed in order of strength of advice from obligation to suggestion: must (also have to) absolute obligation / duty should firm advice or obligation can opportunity / possibility could suggestion might tentative / polite suggestion Task 7. It is essential that (reviewed) 85 Grammar for Academic Writing: Unit 7 � Speculating: Conditionals and modals Writing about the future often involves a combination of predicting, speculating and recommending, as you can see in these extracts from an article about the future of nursing by Professor Kath Melia of the Department of Nursing Studies at iv Edinburgh: It is crucial that we educate nurses who can plan and effect care in a changing social context, and with an ageing population. The shift in emphasis in health care provision to the community is likely to produce a nursing profession in which a more generalised idea of care and nursing practice is more important than specialisation. The education process will have to yield nurses with analytic skills and a capacity to adapt; the graduate nurse with a firm grounding in the ways of community care will be in the lead in this scenario. A more collegial approach might be preferable, with a skill mix which allows nurses with different backgrounds and qualifications to work together in multi-skilled teams to effect patient care. If the medical profession needs assistants, let it find and train them without mounting border-raids on nursing. This task will practise a number of the grammatical and lexical features we have covered in the course units: � a summary of what you did during the course � an evaluation your positive and negative comments � a recommendation for future years would you suggest any changesfi The expression �a major suspect� would probably not be used in formal writing; the others would be perfectly suitable for writing. At the height of the persecution of the Christians of Cordoba, a part of the Christian community protested that the victims were not truly martyrs because they had not been killed by pagans but by Muslims, �men who worship God and acknowledge heavenly laws�. It may have been as early as 717 that mosques were permitted within the walls of Constantinople for the use of Muslim visitors and prisoners of war. If you have been using these Grammar for Academic Writing materials independently, please email your evaluation to Anton. Further help with grammar and vocabulary Here is a list of some useful books and websites, with our comments. Hughes; Cambridge University Press) Like Grammar for Academic Writing, this book aims to develop your understanding of how genre, context and purpose affect grammatical choices in writing. It presents grammatical rules (and exceptions) simply and clearly, and provides plenty of sentence-level exercises. However, it provides rather limited help for students needing to write academic assignments. O�Dell; Cambridge University Press) A guide to the key academic vocabulary used in all fields. Raimes; Cambridge University Press) Very practical guidance on points to notice when editing your own academic writing. As well as covering the usual areas, it comments on differences between spoken and written grammar where necessary. Also includes a useful test to show you which grammatical areas you need to concentrate on. Eastwood; Oxford University Press) A very thorough grammar reference book with clear explanations (there is a good section on articles and related points, for example), but no exercises. A companion volume, Oxford Practice Grammar, by the same author, has exercises but less complete explanations. McCarthy; Cambridge University Press) �The ultimate guide to English as it is really used�, according to the publishers. A large, very comprehensive reference grammar, for both spoken and written usage, based on recent research. Web resources Links to a number of useful grammar websites can be found in the website Using English for Academic Purposes Additional research has expanded our knowledge of previously available treatments. This practice guideline aims to help clinicians optimize care for their patients by providing evidence-based statements that are intended to enhance knowledge and increase the appropriate use of treatments for schizophrenia. Schizophrenia is associated with significant health, social, occupational, and economic burdens as a result of its early onset, and its severe and often persistent symptoms (American Psychiatric Association 2013a). Lost productivity due to unemployment and caregiving each account for approximately one-third of total costs, and direct health care costs account for approximately one-quarter of total costs. Schizophrenia is also associated with increased mortality, with a shortened lifespan and standardized mortality ratios that are reported to be two to four-fold those in the general population (Hayes et al.
Absence of neurological medicine 101 purchase revia line, sensory or physical impairments that directly affect use of spoken language symptoms questionnaire buy cheap revia online, or of a pervasive developmental disorder (F84 treatment yeast infection men order 50 mg revia otc. Absence of neurological symptoms walking pneumonia purchase revia no prescription, sensory, or physical impairments that directly affect receptive language, or of a pervasive developmental disorder (F84. Severe loss of expressive and receptive language skills over the course of a time period not exceeding six months. The disturbance in A significantly interferes with academic achievement or activities of daily living that require reading skills. Not directly due to a defect in visual or hearing acuity, or to a neurological disorder. Possible additional inclusion criterion: For some research purposes investigators may wish to specify: "A history of some level of impairment during the preschool years in speech, language, sound categorization, motor coordination, visual processing, attention or activity control or modulation. The research diagnostic criteria for general reading backwardness would be the same as for specific reading disorder except that criterium A1 would specify reading skills 2 standard error of prediction below the level expected on the basis of chronological age. The validity of the differentiation between these two varieties of reading problems is not unequivocally established but it seems that the specific type has a more specific association with language retardation (whereas general reading backwardness is associated with a wider range of developmental disabilities), and shows a stronger male preponderance. There are also further research differentiations that are based on analyses of the types of spelling errors. Scores on reading accuracy and comprehension, and on arithmetic, that are within the normal range (+ 2 standard deviations from the mean). The disturbance in A significantly interferes with academic achievement or activities of daily living that require spelling skills. Scores on reading accuracy and comprehension, and on spelling that are within the normal range (+ 2 standard deviations from the mean). The disturbance in A significantly interferes with academic achievement or activities of daily living that require mathematical skills. The disturbance in A significantly interferes with academic achievement or activities of daily living. It is common for each of these specific developmental disorders to be associated with some degree of general impairment of cognitive functions, and this mixed category should be used only when there is a major overlap. Thus, the category should be used when there are dysfunctions meeting the criteria for two or more of F80. Presence of abnormal or impaired development before the age of three years, in at least one out of the following areas: (1) receptive or expressive language as used in social communication; (2) the development of selective social attachments or of reciprocal social interaction; (3) functional or symbolic play. Qualitative abnormalities in communication, manifest in at least two of the following areas: (1) a delay in, or total lack of development of spoken language that is not accompanied by an attempt to compensate through the use of gesture or mime as alternative modes of communication (often preceded by a lack of communicative babbling); (2) relative failure to initiate or sustain conversational interchange (at whatever level of language skills are present) in which there is reciprocal to and from responsiveness to the communications of the other person; (3) stereotyped and repetitive use of language or idiosyncratic use of words or phrases; (4) abnormalities in pitch, stress, rate, rhythm and intonation of speech; D. Restricted, repetitive, and stereotyped patterns of behaviour, interests and activities, manifest in at least two of the following areas: (1) an encompassing preoccupation with one or more stereotyped and restricted patterns of interest that are abnormal in content or focus; or one or more interests that are abnormal in their intensity and circumscribed nature although not abnormal in their content or focus. The clinical picture is not attributable to the other varieties of pervasive developmental disorder; specific developmental disorder of receptive language (F80. Presence of abnormal or impaired development at or after age three years (criteria as for autism except for age of manifestation). Qualitative abnormalities in reciprocal social interaction or in communication, or restricted, repetitive and stereotyped patterns of behaviour, interests and activities (criteria as for autism except that it is not necessary to meet the criteria in terms of number of areas of abnormality). That is, abnormal or impaired development is evident only at or after age three years. Qualitative abnormalities in reciprocal social interactions or in communication, or restricted, repetitive and stereotyped patterns of behaviour, interests and activities (criteria as for autism except that it is not necessary to meet the criteria in terms of number of areas of abnormality). That is abnormal or impaired development is evident only at or after the age of three years. Apparently normal prenatal and perinatal period and apparently normal psychomotor development through the first six months and normal head circumference at birth. Deceleration of head growth between five months and four years and loss of acquired purposeful hand skills between six and 30 months of age that is associated with concurrent communication dysfunction and impaired social interactions and appearance of poorly coordinated/unstable gait and/or trunk movements. Development of severely impaired expressive and receptive language, together with severe psychomotor retardation. Stereotyped midline hand movements (such as hand wringing or washing) with an onset at or after the time that purposeful hand movements are lost. The presence of normal age-appropriate skills in communication, social relationships, play, and adaptive behaviour at age two years or later is required for diagnosis. A definite loss of previously acquired skills at about the time of onset of the disorder. The diagnosis requires a clinically significant loss of skills (and not just a failure to use them in certain situations) in at least two out of the following areas: (1) expressive or receptive language; (2) play; (3) social skills or adaptive behaviour; (4) bowel or bladder control; (5) motor skills. Qualitatively abnormal social functioning, manifest in at least two of the following areas: (1) qualitative abnormalities in reciprocal social interaction (of the type defined for autism); (2) qualitative abnormalities in communication (of the type defined for autism); (3) restricted, repetitive and stereotyped patterns of behaviour, interests and activities including motor stereotypies and mannerisms; (4) a general loss of interest in objects and in the environment. The disorder is not attributable to the other varieties of pervasive developmental disorder; acquired aphasia with epilepsy (F80. Severe motor hyperactivity manifest by at least two of the following problems in activity and attention: (1) continuous motor restlessness, manifest in running, jumping and other movements of the whole body. Repetitive and stereotyped patterns of behaviour and activity manifest by at least one of the following: (1) fixed and frequently repeated motor mannerisms: these may involve either complex movements of the whole body or partial movements such as hand-flapping. A lack of any clinically significant general delay in spoken or receptive language or cognitive development. Diagnosis requires that single words should have developed by two years of age or earlier and that communicative phrases be used by three years of age or earlier. Self-help skills, adaptive behaviour and curiosity about the environment during the first three years should be at a level consistent with normal intellectual development. However, motor milestones may be somewhat delayed and motor clumsiness is usual (although not a necessary diagnostic feature). Isolated special skills, often related to abnormal preoccupations, are common, but are not required for diagnosis. Qualitative abnormalities in reciprocal social interaction (criteria as for autism). An unusually intense circumscribed interest or restricted, repetitive, and stereotyped patterns of behaviour, interests and activities (criteria as for autism; however it would be less usual for these to include either motor mannerisms or preoccupations with part- objects or non-functional elements of play materials). The disorder is not attributable to the other varieties of pervasive developmental disorder; schizotypal disorder (F21); simple schizophrenia (F20. Eventually, assessment instruments should develop to the point where it is possible to take a quantitative cut-off score on reliable valid and standardised measures of hyperactive behaviour in the home and classroom, corresponding to the 95th percentile on both measures. Demonstrable abnormality of attention, activity and impulsivity at home, for the age and developmental level of the child, as evidenced by (1), (2) and (3): (1) at least three of the following attention problems: (a) short duration of spontaneous activities; (b) often leaving play activities unfinished; (c) over-frequent changes between activities; (d) undue lack of persistence at tasks set by adults; (e) unduly high distractibility during study. Demonstrable abnormality of attention and activity at school or nursery (if applicable), for the age and developmental level of the child, as evidenced by both (1) and (2): (1) at least two of the following attention problems: (a) undue lack of persistence at tasks; (b) unduly high distractibility, i. The evidence may be any of the following: (1) direct observation of the criteria in G1 or G2 above, i. Does not meet criteria for pervasive developmental disorder (F84), mania (F30), depressive (F32) or anxiety disorder (F41). Specification for possible subdivisions Authorities differ on the best way of subdividing the conduct disorders, though most agree that they are heterogeneous. For determining prognosis, the severity (indexed by number of symptoms) is a better guide than the precise type of symptomatology. The best-validated distinction is that between socialized and unsocialized disorders, defined by the presence or absence of lasting peer friendships. However, it seems that disorders confined to the home may also constitute a meaningful subvariety and a category is provided for this purpose. It is clear that further research is needed to test the validity of all proposed subdivisions of conduct disorder. However, in addition to these categorizations it is recommended that cases be described in dimensional terms according to their scores on three dimensions of disturbance: (1) hyperactivity (inattentive, restless behaviour); (2) emotional disturbance (anxiety, depression, obsessionality, hypochondriasis); and (3) severity of conduct disorder (indexed by number of items from G1 above). Definitely poor relationships with peer group as shown by isolation, rejection or unpopularity and by a lack of lasting close reciprocal friendships. Presence of three of more symptoms from the criterion list above, of which at least three must be from items 9-24. At least one of the symptoms from items 9-24 must have been present for at least six months. Presence of four or more symptoms from the criterion list above, of which no more than two from items 9- 24. The symptoms in B must be maladaptive and inconsistent with the developmental level. The general criteria for conduct disorder (F9l) or oppositional defiant disorder (F91. The general criteria for conduct disorder (F91) or oppositional defiant disorder (F91.
Awareness and reactions of young stuttering children aged 2�7 years old towards their speech disfluency medicine hat jobs discount revia 50mg amex. Parent perceptions of the impact of stuttering on their preschoolers and themselves treatment of diabetes purchase genuine revia. Peer victimization: Manifestations and relations to medicine z pack purchase generic revia from india school adjustment in kindergarten 98941 treatment code best buy for revia. Graham (Eds), Peer harassment in school: the plight of the vulnerable and victimized (pp. KiddyCat: Communication attitude test for preschool and kindergarten children who stutter. A comparative investigation of the speech- associated attitude of preschool and kindergarten children who do and do not stutter. Factors associated with negative attitudes toward speaking in preschool-age children who do and do not stutter. Preliminary study of self-reported experience of physical aggression and bullying of boys who stutter: Relation to increased anxiety. Communication apprehension and accumulated communication state anxiety experiences: A research note. Communication apprehension and self-perceived communication competence in adolescents who stutter. The social and communication impact of stuttering on adolescents and their families. Psychological health and coping strategies of adolescents with chronic stuttering. Psychiatric disorder, impairment, and service use in rural African American and white youth. A parent-report measure of children�s anxiety: Psychometric properties and comparison with child-report in a clinic and normal sample. Anxiety in 11-year- old children who stutter: Findings from a prospective longitudinal community Sample. The speech-associated attitude of children who do and do not stutter and the differential effect of age. The relationship between communication attitude and emotion of children who stutter. Speech-associated attitudes in children who stutter and in children who do not stutter. Study of the communication attitude of Slovenian children who do and do not stutter. Communicative ability conceptions among children who stutter and their fluent peers: A qualitative exploration. The impact of adolescent stuttering and other speech problems on psychological well-being in adulthood: Evidence from a birth cohort study. A preliminary study of self-esteem, stigma, and disclosure in adolescents who stutter. Self-reported experience of bullying of students who stutter: Relations with life satisfaction, life orientation, and self-esteem. Comparing acceptance and rejection in the classroom interaction of students who stutter and their peers: A social network analysis. A cross-sectional investigation of the correlates of bullying and anxious depression. Preliminary examination of the relationship between anxiety disorders in adults and self-reported history of teasing or bullying experiences. The relationship between memories for childhood teasing and anxiety and depression in adulthood. Twenty years research on peer victimization and psychosocial maladjustment: A meta-analytic review of cross-sectional studies. The relationship between anxiety disorders in adults and recalled childhood teasing. Adult recall of having been bullied in attenders of an anxiety disorder unit and attenders of a dental clinic: A pilot controlled study. Long-term consequences of childhood bullying in adults who stutter: Social anxiety, fear of negative evaluation, self-esteem, and satisfaction with life. Teasing/bullying experienced by children who stutter: Toward development of a questionnaire. Sociodynamic relationships between children who stutter and their non- stuttering classmates. Parental psychopathology, parenting styles, and the risk of social phobia in offspring: A prospective-longitudinal community study. Prevalence of psychiatric disorders in children with speech and language disorders. Fourteen-year follow-up of speech/language-impaired and control children: Psychiatric outcome. Fourteen-year follow-up of children with and without speech/language impairments: Speech/language stability and outcomes. This has prompted statements that any such client with significant anxiety, regardless of whether it amounts to a diagnosable psychological 1,2 problem, requires clinical management. That being said, not all clinicians will have the necessary training or experience to manage social anxiety with stuttering clients. Treatment of anxiety is fundamentally the professional domain of clinical psychologists and psychiatrists. Speech-language pathology professional preparation programs around the world vary in the extent to which they incorporate anxiety management training. However, alone, they are not a qualification to diagnose and manage anxiety disorders. Clinical psychologists and psychiatrists typically diagnose an anxiety disorder after a period during which they formally test, interview, and generally become familiar with a client. Such an assessment process would cover domains in addition to anxiety that are related to it, such as depression and stress. As noted during the previous lecture, adults seeking treatment for stuttering often are affected by social anxiety disorder. An overview is available 3 of clinical measures for that specific disorder that clinical psychologists can use. The following measures for social anxiety are suitable for administration by speech-language pathologists; they require no formal psychology qualifications to administer. A specific caveat is needed for speech-language pathologists about measuring the anxiety of children, because it is a lot different to measuring anxiety with adults. One complicating factor is the possible limitations of child report about anxiety. Because of this, it is generally agreed that parent reports are essential input for assessing anxiety with children. Clinical psychologists administer tests, observe children, and interview them and their parents�and sometimes teachers�to form a diagnosis. It would be prudent for speech-language pathologists only to screen children for anxiety to determine whether referral to a clinical psychologist is necessary. The scale can be downloaded from the website of the 4 Australian Stuttering Research Centre, and is presented in Appendix One of this lecture. To complete the scale, for each of those thoughts the client indicates how frequently it occurs on a scale of 1 to 5: 1 = never or not at all, 2 = rarely or a little, 3 = sometimes or somewhat, 4 = often or a lot, 5 = always or totally. To supplement this basic scale, there are two other scales that measure how much clients believe each thought, and how anxious each thought makes them feel. For example, clinicians could adapt certain scale items to ask a client during an interview: �have you ever thought that people would doubt your ability because you stutterfi That may not be so advisable with younger adolescents, and the scale is probably of limited use with school-age children. The mean score differences between participants with and without an anxiety disorder are presented also. The six items are able to accurately reproduce the total score for each of the three subscales. However, this does not mean that a score below the fifth decile excludes a clinically significant anxiety problem.
Purchase 50 mg revia with amex. Multiple Sclerosis (MS) Clearly Explained - MADE EASY.