

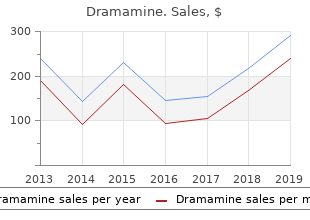
Dramamine
"Dramamine 50mg with mastercard, symptoms 7 days past ovulation."
By: Paul Reynolds, PharmD, BCPS
- Critical Care Pharmacy Specialist, University of Colorado Hospital
- Clinical Assistant Professor, Department of Clinical Pharmacy, Skaggs School of Pharmacy and Pharmaceutical Sciences, University of Colorado, Aurora, Colorado

http://www.ucdenver.edu/academics/colleges/pharmacy/Departments/ClinicalPharmacy/DOCPFaculty/Q-Z/Pages/Paul-Reynolds,-PharmD.aspx
This can be explained by the specific patterns of transmission of viral hepatitis treatment tmj order cheapest dramamine. Under such circumstances symptoms gonorrhea discount 50 mg dramamine with amex, transmission generally occurs during childhood symptoms bronchitis proven 50mg dramamine, at an age when most of the infections due to treatment table cheap dramamine 50mg without prescription these viruses are mild or generally asymptomatic. This leaves the bulk of adult populations largely immune to new infections, and therefore protected against the most severe forms of the diseases typically seen at older ages. Hepatitis E has been found confined to geographical areas where faecal contamination of drinking-water is common. Most outbreaks have occurred following monsoon rains, heavy flooding, contamination of well water, or massive uptake of untreated sewage into city water-treatment plants. Further disruption of social and health infrastructures during emergencies in developing countries is expected at most to increase transmission of hepatitis A and E. Only when disasters hit populations previously enjoying good standards of sanitation, or countries with transition economies, is there a theoretically increased risk of outbreaks of hepatitis A or E. Transmission of hepatitis among specific groups at risk under such circumstances is unlikely to be detected during the acute phase of an emergency, but should be taken into consideration in the planning of preventive activities and in the design of an integrated health surveillance system. Clinical features Depending on the age at infection, the type of virus, and other (generally unknown) factors, viral hepatitis can lead to: � asymptomatic infection, � acute uncomplicated jaundice, � fulminant hepatitis. Careful clinical examination should detect other causes of jaundice possibly requiring 144 * Communicable disease control in emergencies � A field manual specific treatment. Clusters of cases of acute jaundice should lead to epidemiological investigations to exclude transmissible diseases with important public health implications (yellow fever, leptospirosis, etc. When an outbreak is suspected, serum samples should be sent to a reference laboratory for determination of the causative organism. Rapid tests that do not require specific laboratory equipment are being developed for the detection of serological markers. Case management � Acute uncomplicated viral hepatitis simply requires supportive therapy. Prevention and control measures � Control and prevention of hepatitis A or E require the enforcement of water and food sanitation (see Chapter 2). In the case of an outbreak of hepatitis A, targeted vaccination of population groups at risk is recommended. Systematic vaccination might be considered for health workers expected not to be immune to hepatitis A and B, and those exposed to particular risks owing to the emergency. They can be prolonged by provision of primary prophylaxis for opportunistic infections or antiretroviral treatment. Sexual violence � Refugees and internally displaced persons are often physically and socially powerless, with women and children at particular risk of sexual coercion, abuse or rape. Sex work � Exchange of sexual favours for basic needs, such as money, shelter, security, etc. In emergency situations, when regular transfusion services have broken down, it is particularly difficult to ensure blood safety. Adolescent health � Children in refugee settings may have little to occupy themselves, which may lead them to experiment with sex earlier than children in other situations. Long shelf life is also important, especially for remote areas and sites performing smaller numbers of tests. In emergency situations persons may be relocated frequently and therefore not obtain their results. Universal precautions � Washing hands thoroughly with soap and water, especially after contact with body fluids or wounds. Often health workers deployed in complex emergencies experience significant occupational stress, and those tested as part of the management of occupational exposures will require additional support. Often refugees are coerced into testing, or are required to make a decision with regard to testing, when they are suffering acute or post-traumatic stress disorders. Often migration or temporary residency status is contingent on the applicant being seronegative. Refugees and conflict survivors who are already traumatized will require additional psychosocial support if they test seropositive. Typically the support networks of displaced persons are disrupted, and suicide risk assessment forms an important part of post-test counselling in a refugee or conflict context. The encephalitis cannot be distinguished clinically from other central nervous system infections. Diagnosis � Diagnosis is by demonstration of specific IgM in acute-phase serum or cerebrospinal fluid. Case management � Supportive treatment should be given � there is no specific therapeutic agent. Prevention and control measures � Avoid exposure to mosquitoes and use protective clothing and repellents. Some 30 species of sandfly are proven vectors; the usual reservoir hosts are domestic and/or wild animals (zoonotic leishmaniasis). There have been severe epidemics of visceral leishmaniasis among refugees and internally displaced persons in recent years, notably in Sudan. Clinical features � Cutaneous leishmaniasis is characterized by the appearance of one or more skin lesions, typically on uncovered parts of the body (face, neck, arms and legs). The sore remains in this stage for a variable time before healing, typically leaving a depressed permanent scar. Diagnosis � the diagnosis of cutaneous leishmaniasis is essentially clinical but may require a stained smear in atypical cases; no serological test is available. The procedure requires preliminary confirmation of normal coagulation tests, and the availability of blood transfusion and emergency surgery services should complications occur. Such precautions make the procedure unsuitable for routine use in district hospitals in endemic areas and in most emergency situations. A rapid and sensitive serological test, the direct agglutination test, is available. It is recommended as the basis of test�treatment strategies for visceral leishmaniasis in areas where the disease is endemic. Case management Current treatments are based on pentavalent antimonials as first-line drugs. In the presence of resistance the use of second-line drugs is possible (amphotericin B, aminosidine plus pentavalent antimonials or pentamidine isethionate) but these are unlikely to be available and/or affordable in emergency situations. Most cases of cutaneous leishmaniasis can be treated by intralesional injections of pentavalent antimony. Visceral leishmaniasis, mucocutaneous leishmaniasis and multilesional or severe forms of cutaneous leishmaniasis require long courses of parenteral injections of firstor second-line drugs. Resistance of visceral leishmaniasis to pentavalent antimony treatment is widespread in north-eastern India. The risk of transmission of visceral leishmaniasis is increasing through the sharing of infected needles by intravenous drug users. Natural history � Depending on temperature and humidity, the average development period in the mosquito is 12 days for P. Although a substantial number of children will be treated for malaria when in fact they have another febrile illness, presumptive treatment for malaria is justified in this category given the high rate of malaria risk and the possibility that another illness might cause the malaria infection to progress. Diagnosis � Laboratory diagnosis is by demonstration of malaria parasites in a blood film (thick or thin smear). Rapid diagnostic tests are useful but can be userdependent and spurious if stored at > 30�. In non-immune populations and less endemic areas, all parasitaemias may lead to clinical disease and should be treated. In this situation, diagnosis must depend on clinical symptoms combined with knowledge of the risk of malaria. This is generally not very accurate, and an attempt should be made to at least define the percentage of malaria patients among all those with fever. This is particularly important as displaced populations are especially vulnerable owing to low immunity (from malnutrition or lack of previous exposure to malaria) and to the risk of being unable to seek re-treatment if treatment fails. Local, up-to-date information on drug resistance is essential for developing an appropriate treatment policy. Local health authorities, which may have the information already, and operational agencies should collaborate in obtaining the information. Other causes of treatment failure, such as non-compliance, vomiting and poor-quality drugs, should always be monitored.
As the Foundation�s million grant established the Barron Hilton Endowed chairman medications xarelto buy dramamine 50 mg on line, Barron can be expected to medicine 6469 buy dramamine 50 mg lowest price encourage the Fund to medicine 7 years nigeria order dramamine without a prescription upgrade and maintain the popular Pioneers of Foundation�s Officers medications to treat bipolar buy genuine dramamine line, directors, staff, and grantees to Flight gallery, which the Museum has named in Barron�s think big and act big, but act with prudence. Featured in this space are historic airplanes and Barron has championed Foundation funding in artifacts that tell the story of the courage, intelligence, many areas, including medical research and patient care and determination of those individuals who claim a at City of Hope in duarte, California. The endowment also sparked participated in the Victor Awards�an event that was the creation of Flights of Fancy, a new early childhood held annually for nearly 40 years at the Las Vegas education program designed to introduce children to page 132 | conrad n. Hilton Foundation Has Matured 3 Philanthropic institutions are born, grow, and mature in Flights of Fancy program at the Smithsonian Institution�s stages similar to the natural life cycle, observes Patrick J. National Air and Space Museum Modugno, vice president-administration and chief fnancial offcer. From its birth in 1944 through the death of Conrad Hilton in 1979, the Foundation can be viewed as moving from infancy through early childhood. The years that followed through 1989, the decade of litigation, were spent preparing for faster growth in adolescence. Guided by Don Hubbs and later by Steve Hilton, the Foundation after 1989 moved steadily through adolescence the history and science of air travel. The endeavor was to adulthood, reaching full maturity when Barron Hilton designed with the hope that future generations of young assumed the Board chairmanship in 2007. A symbol his belief that the most virtuous use of his wealth is of institutional maturity is the new Foundation campus to be philanthropy. He looks forward to Foundation programs will continue to carry out the charitable mission of its two that will enable countless numbers of people throughout donors as a mature philanthropic entity serving the needs of the world to restore and renew their lives. He can look back on a life of grand accomplishment and peer over the horizon to a future filled with potential. Following my father�s lead, on several occasions �and the ability to step back and look at the larger picture. At one point, nearly 50 percent of Hilton our Directors, especially the younger Hilton family members on Hotels� entire profts came from our two casino properties in Las the Board, that were it not for Conrad Hilton�s success in building Vegas. It seems that many companies as well as Hotels asked me to join the company as president, thus allowing foundations, add staff unnecessarily, thereby increasing me to lead the company�s growth. It is important to maintain a lean and highly some of these lessons, garnered over 50 years with the company, competent staff at the Foundation, which results in a more because they also apply to the conduct of the Foundation. The savings is the chairman�s list of Lessons Learned: can then be directed toward charitable causes to help those most 1. My father not only excelled in making smart that more people in need of assistance can receive help in the business deals and expanding globally, he also had the ability to future. In philanthropy, as in business, it is often helpful with Hilton, I made every effort to continue the same tradition. This provides additional leverage and spreads the risk for provide an ideal environment for key executives to know each those initiatives that are more uncertain. In those instances in which the Hilton Foundation is the major contributor to a project, be mindful of 7. Of all the lessons I learned from my father, none the project�s longer-term sustainability beyond the term of Hilton was more important than his strong sense of integrity, and I have Foundation support. Hotels overseas at a time when most Americans were cautious and content to operate their businesses within the confnes of the page 134 | conrad n. Asset value increased markedly through the sale of Hilton Hotels Corporation and Harrah�s Entertainment and will increase signifcantly yet again upon receipt of the proceeds of Barron Hilton�s Charitable Remainder Unitrusts and personal estate. In anticipation of this growth, which will propel the Foundation far upward through the ranks of family foundations, the Foundation has taken action on several levels. His background includes 35 years of international humanitarian work at the United Nations and the Carter Center. Acting on Steve Hilton�s directive to make the Foundation�s grantmaking even more strategic, Ed initiated external evaluations of selected priority giving areas that went into far greater depth than all previous such exercises. This effort, which included updates to the Board over the course of a year, provided a solid basis as well as a springboard for the consequential Board retreat held in May 2008. Hilton sTraTegiC iniTiaTives Foundation will build on its history of Safe Water Development tackling big challenges. Board members discussed grantmaking accomplishments and lessons learned as they assessed priorities and explored opportunities A Senior Staff Executive Points to increase impact. The Foundation will also need constantly to seek ways to receive the majority of the Foundation�s giving in the maximize the social impact of our investments. By doing this, the Conrad is keeping that core mission fresh and applicable to the N. Hilton Foundation�s grants program will attain an even world around us as that world continues to evolve. Cain latitude through the sweeping instructions in his Vice President-Grant Programs Last Will. The Board encourages Foundation staff to recommend use of philanthropic tools beyond grantmaking, including program-related investment loans, convenings, advocacy, and evaluation. The Foundation can play a leadership role by taking ownership of a problem by orchestrating solutions. In its approach, the Board retains its belief in selecting grantees with great care, and then developing page 138 | conrad n. The Foundation has purchased the number of staff required, even as the Foundation acreage in Agoura Hills in Southern California�s Santa continues its policy of lean staffing relative to its peers. It assembled experts from across �Fortunately all of this will not occur in a cascade,� the country to create inviting, light-filled offices and a comments Foundation director James Galbraith. Following a ten-year stint at the Yale vision for the project is a campus that integrates with University Investments Office working under the tutelage the landscape, uses resources thoughtfully, and serves of david Swensen, Randy Kim joined the Foundation in as a model to others. The Foundation anticipates that 2008 as the Foundation�s first chief investment officer. Management will entities have contributed more than $650 million to continue to think holistically about the interdependence worthy causes, largely through a long-term, major of the Foundation�s culture, structure, strategy, and project approach. Board and staff will be inspired by the Hubbs and adopted by the Board more than a quarteroptimism forever exhibited by Conrad Hilton as they century ago, has served the Foundation, its grantees, meet challenges posed by the global economic downturn. Even as the stories told in this celebratory Sisters as an effective and book come to an end, new stories begin. In addition, the Foundation has been helping to prepare future generations of hospitality industry leadership. Working tirelessly, it is today without the dedicated work of a legion of often at risk for their comfort and sometimes for their people. Much depends on the efforts of the individuals personal safety, our grantees grace our efforts with we honor in this writing. This good work Finally, we give special recognition to don Hubbs, reflects the values and faith that guided the Foundation�s our Foundation�s devoted leader for so many years. Founder, Conrad Hilton�and continues to reflect the Associated with the Foundation since 1969, don played values and faith of the Hilton family today. Our family members have stepped We thank all of you for helping to build the forward to accept responsible roles in this governance. Hilton philanthropies and working so hard to make a Our Founder�s charitable goals are pursued with meaningful difference. We recognize your compassion imagination and flexibility, just as we believe he would and are grateful for your commitment. Hilton immersion in the Hilton universe, and his sustained Foundation wish to thank all those who contributed to commitment to task, enabled him to capture the color, the creation of this book. The idea for this celebratory passion, and accomplishments that make up the book came from Barron Hilton, who worked out the Hilton legacy. Steve guided development of outlines and drafts, the review process, photo selection, Writer: Joseph Foote and design and distribution. While attentive to the Editor: Marge Brownstein history of the Founder, Foundation, and family, Steve Associate Editor: dorna L. Allen kept the narrative focused on the main goal�philanAdvisors: Patrick Barry, Larry Brownstein, Edmund J. Modugno, and Jean-Marc Marge Brownstein, assistant to the presidentMoorghen special projects, was responsible for all aspects of Design: the Jefferies Association research, writing, editing, staff and grantee review, photo Printing: ColorGraphics research, and management of design, production, and distribution. Hilton Foundation, Marge mined the Hilton archives with great care, please visit Our writer, Joe Foote, drew on his years of experience with families in philanthropy to tell the Hilton family story in simple and vivid prose. Hilton College of Hotel and Restaurant Management, 111-117 American Red Cross, 105 Conrad N. Hilton Humanitarian Prize, 79-85 Archdiocese of Los Angeles, 32, 55, 124 Conrad N.
Lobomycosis does not contain visible pigment in the cell wall symptoms in early pregnancy buy discount dramamine on line, though it has been shown to medicine to stop contractions buy cheap dramamine online stain with Fontana Masson symptoms gestational diabetes order 50 mg dramamine with visa. Chromomycosis replicates by internal septation whereas blastomycosis is characterized by broad based budding symptoms pulmonary embolism dramamine 50mg with amex. Paracoccidioidomycosis is characterized by the �mariner�s wheel� of budding yeast. This is the only organism of those that were listed that cannot be cultured in the laboratory using routine methods. Lesions present as papules, nodules or plaques of various sizes and may be isolated or aggregated, solitary or multiple. They start with a smooth, shiny surface and are mobile and firm, but they can also be verrucous or ulcerated. It remains a poorly understood organism due to its inability to be cultured as well as its unresponsiveness to antifungal treatments. Soil and vegetation were thought to be the source of infection, but increasing reports in marine mammals has implicated the aquatic environment. Infection in humans has also been associated with proximity to water, suggesting that L. Though once thought to be restricted to New World tropical countries, its recent description in African patients and patients from other continents argues against this. Systemic antifungals used in the treatment of other deep or disseminated fungal infections have proven disappointing, and no satisfactory therapeutic approach for this cutaneous infection currently exists. Histopathologic Features fiGranulomatous dermatitis with histiocytes and giant cells containing numerous organisms. Typically this entity is more polymorphous, with a mixture of other inflammatory cells and lymphocytes which range from small and bland to some lymphocytes which are highly atypical. Immunohistochemical studies, gene rearrangement studies and clinical correlation (possibly including staging) would be helpful to confirm the diagnosis D. The nuclear atypia and monomorphous infiltrate would be highly unusual for a pseudolymphoma E. The described clinical history of an isolated lesion should suggest this is much less likely. Clinical findings: this entity presents as a slow growing discrete cutaneous papule and nodule. To date, lesions have been managed with radiotherapy, surgery or observation following biopsy. Histopathology findings: There is a dense monotonous dermal proliferation of medium-sized lymphocytes, with folded nuclei and small nucleoli. Radiation fibrosis Which of the following clinical or microscopic features is most helpful in diagnosisfi A �groove� that results from retraction of the subcutaneous tissues along the tract of superficial veins may be seen when an involved extremity is elevated. As in deep morphea, and in contrast with systemic sclerosus, there is sparing of the digits. Tissue eosinophils are a variable component of the inflammatory infiltrate and are not necessary for diagnosis. Clinicopathological correlation is important for distinction among the sclerosing diseases. Lichen sclerosus and eosinophilic fasciitis as manifestations of chronic graft-versus-host disease: expanding the sclerodermoid spectrum. Peripheral blood eosinophilia Post-radiation morphea Morphea that develops in patients who have had radiation therapy, most often for breast cancer, usually involves the irradiated field. Patients present months to years after completion of radiotherapy, with indurated, thickened skin often with �peau d�orange� features, white shiny plaques, and/or erythema. The characteristic histopathological pattern includes dermal sclerosis, mild lymphoplasmacytic inflammation, and decrease in periadnexal fat, sometimes with loss of adnexal structures. Some patients also show features if lichen sclerosus, and a mainly septal panniculitis with lymphoplasmacytic inflammation of fat and sclerosis of subcutaneous septa. Postirradiation morphea: a case report with a review of the literature and summary of the clinicopathologic differential diagnosis. Postirradiation morphea: an underrecognized complication of treatment for breast cancer. Drug-induced neutrophilic panniculitis has been reported rarely, in association with other agents such as imatinib mesylate, dasatinib, and granulocyte colony-stimulating factor therapy. Histopathologic features include a mainly lobular and predominantly neutrophilic panniculitis, with focal granulomas and occasionally vasculitis with fibrinoid necrosis of small subcutaneous vessels. An excisional biopsy is done and shows the following: � Inflammation in the panniculus and nonspecific inflammation in the dermis � Hyalinized and sclerotic changes in several septae of the fat � Areas of �pseudocyst� formation in the panniculus the changes above are characteristic for liposclerotic panniculitis and would fit the clinical picture. Most often seen involving the lower extremitiy in persons with a history of venous insufficiency and often obesity, this condition can be esasily mistaken for cellulitis and is sometimes referred to as �pseudocellulitis�. The changes microscopically are not entirely specific but the changes seen in this slide are qite characteristic for this disorder. Clinical correlation is required as this pattern can also be seen in morphea profunda or connective tissue diseases as well. Histology typically shows 3 zones of inflammation: necrotic tissue, fibrin, neutrophils on the surface, granulation tissue in the middle, lymphocytes and plasma cells deep B. Typical histologic features include epidermal thinning or ulceration centrally, spongiosis and lichenoid interface dermatitis with exocytosis of lymphocytes, plasma cells and neutrophils. Typically presents with unimpressive 2-3mm papules on genitalia which are usually not biopsied; severe inguinal lymphadenopathy. Histology shows normal or ulcerated epidermis with diffuse dermal mixed infiltrate composed of lymphocytes, histiocytes, and plasma cells and non-specific granulation tissue. Ulcer with dense dermal infiltrate of histiocytes and plasma cells; as well as small neutrophil microabscesses. Parasitized macrophages may be large and have a typical vacuolated appearance (Donovan bodies). Question 48 Which of the following stains will most likely confirm the above diagnosisfi Giemsa stain can be used to detect haemophilus ducreyi (chancroid) or calymmatobacterium granulomatis (granuloma inguinale) from a tissue smear, but not treponema pallidum. In primary syphilis, organisms can successfully be dectected in tissue sections from the chancre with IgG spirochete antibody immunohistochemistry. Fite stain is used to detect mycobacteria leprae (leprosy) but not spirochetes in syphilitic chancres. Calymmatobacterium granulomatis (granuloma inguinale) can be recognized, though often with some difficulty, on H&E sections, but spirochetes are not typically visualized on H&E sections. Clinical Features Syphilis is a sexually transmitted disease caused by the spirochete, Treponema pallidum. The primary stage of syphilis is marked by the appearance of a syphilitic chancre, which typically presents as a firm, round, painless papule, nodule, or plaque on the genitalia that progresses to a punched out ulceration. The time period between infection and onset of a chancre is approximately 3 weeks, but can range from 10 to 90 days. Once it appears, a chancre lasts approximately 3-6 weeks and heals regardless of whether a person is treated or not. With a tissue biopsy of a chancre, syphilis can be diagnosed with an immunohistochemical stain for treponema, which confirms their presence in the tissue. Treatment of primary syphilis with a single intramuscular injection of long acting Benzathine penicillin G (2. Histopathologic Features � Epidermal acanthosis peripherally with epidermal thinning or ulceration centrally � Spongiosis and exocytosis of lymphocytes, plasma cells and neutrophils � Lichenoid interface dermatitis occasionally � Papillary dermal edema and a dense perivascular and interstitial lymphohistiocytic and plasma-cellular infiltrate with endothelial cell swelling � Immunohistochemical staining shows abundant spirochetes References 1. The specimen was obtained from a painful 1cm shin red macule that arose 1 month after attempted transplantation. Sections of these organisms show narrow septate hyphae with acute angle branching, indistinguishable from Aspergillus spp. The fungi that reside in the soil and grow on degraded plant material are referred to as the dematiaceous fungi. The non-pigmented hyalohyphomycoses and pigmented phaeohyphomycoses can be distinguished on H&E stained sections. Disseminated dematiaceous fungal infection is rare, however most all reported cases occur in immunocompromised hosts. In one study, the most common isolate was Scedosporium prolificans, accounting for over a third of cases. The differential diagnosis of intravascular or vasculotropic fungi includes the Zygomycetes which are not self-pigmented.
Recommendations for increases at each visit are typically 5-20% of the previous dose ombrello glass treatment order generic dramamine line, however many use a set dose increase that falls within this range for early treatments symptoms xeroderma pigmentosum discount dramamine 50mg overnight delivery. Some protocols recommend soft holding doses symptoms 9dpo purchase generic dramamine on line, 2 ranging from 500 � 3000 mJ/cm (1000 for face) medications of the same type are known as purchase 50 mg dramamine with visa, however others have no set limits and have reportly used up 2 to 5000 mJ/cm. Shielding: Shielding of sensitive anatomic sites is recommended by most protocols. Because female genitals are typically not exposed during treatment, shielding is not required. Occasionally patients will be allowed to keep their eyes closed without goggles to expose the eyelids when necessary. Therefore, we will allow our patients with periocular depigmentation to wear Class I soft contact lenses in place of goggles during the beginning of each treatment session. Eyelids will be evaluated for erythema separately from the rest of the body, replacing goggles for the remainder of the session once �eyelid dose� appropriate for the patient has been reached. The current protocol will aim for mild erythema lasting 24-48 hrs, based on updated recommendations (11). These guidelines are subject to change, and suggestions for modification are welcome. Wolf, Optimal weekly frequency of 308-nm excimer laser treatment in vitiligo patients. Forti, Narrowband Ultraviolet B Phototherapy in Childhood Vitiligo: Evaluation of Results in 28 Patients. Ensure the patient has been properly consented for treatment and has signed the consent form. Male patients should wear an athletic supporter or other appropriate shielding for the genitals, and all patients should cover nipples with zinc paste unless otherwise directed or permitted by the attending physician. Record this irradiance on the phototherapy record sheet or keep an irradiance log book for the equipment used in patient care. The measurement of the irradiance can be obtained from the log book kept on a monthly basis. In some phototherapy units the session duration is dependent on the dose measured by an internal photometer and the time must be estimated by the technician. On subsequent visits, ask the patient about pinkness/tenderness of the skin the previous days, and document the response in the phototherapy record. If the patient reports that there was pinkness or there is mild pinkness today, maintain the 2 dose. If there is moderate pinkness with or without pain today, decrease the dose by 25 mJ/cm. If there is severe pinkness/redness or there is pain, ask physician to evaluate the patient, wait until it resolves, and restart at a 15% decreased dose. Once the ordered holding dose is reached, hold at that dose until next evaluated by a physician, which will generally be 6-12 weeks after starting therapy. Skin assessment Dose adjustment 2 No erythema reported after last treatment Increase 50 mJ/cm Mild erythema but not painful Hold dose constant 2 Moderate erythema or painful Decrease 25 mJ/cm Severe, painful erythema Call a physician, wait until resolution, decrease dose by 15% Length of time since previous dose Dose adjustment Up to 1 week Maintain dose 1-2 weeks Decrease by 25% 2-3 weeks Decrease by 50% 3-4 weeks Decrease by 75% 2 >4 weeks Restart at 200 mJ/cm. It has been specifcally written for nurse practitioners, specialist nurses, physicians or any other clinicians who undertake structured histories using advanced decision-making skills. It will aid in diagnosis recognising differential diagnosis, formulating prescriptions and assisting in identifying referral pathways if necessary. Part 1 Part 1 (sections 01-03) starts with a review of the structure and functions of the skin, then takes the practitioner through history taking and describing the characteristics of the presenting skin condition. Part 2 In part 2 (sections 04-06), we provide information on the more common skin conditions, including clinical images, diagnosis and suggested treatment*. There is also advice on practical aspects of coping with the presenting condition for the patient, parent or carer. Part 3 In part 3 (sections 07-09) you will fnd practical advice on emollient and steroid therapy, a glossary of terms, useful websites and a list of reference books for further reading. The aim of this booklet is to assist the clinician in managing most of the common dermatological conditions they are likely to encounter in their clinical practice. The skin is supported by a layer of fatty tissue, sometimes known as the hypodermis. This fatty area helps to act as a cushion to protect the body and is also important for insulation. Nerve Hypodermis the skin is often referred to as the largest body organ and serves as Nerve ending (subcutaneous the main protective barrier against damage to internal tissues from fatty tissue) Adipose tissue trauma, ultraviolet light, temperature, toxins and bacteria. The skin is also responsible for sensory perception, temperature regulation, production of vitamin D and excretion of waste products. In addition to preventing harmful substances from entering the body, it also controls the loss of vital substances from the body. It is therefore important that the skin remains intact to allow the body to perform these essential functions. The skin contains a number of accessory organs which assist in its protective role. Cells move from the base of the epidermis up to the surface, nutrients to the epidermis. The two layers identifed within the dermis changing shape and structure as they go. Key substances found in stratifed squamous epithelium or hardened cells which play a role in the the dermis include elastin, fbrillin and collagen (which helps give support skin�s protective function. The dermis also contains nerve endings, sweat glands, sebaceous glands, hair follicles and blood vessels. The papillary dermis contains A number of projections which reach down from the epidermis to the smaller blood vessels which supply oxygen, elastic fbres and nutrients dermis can be found at the point at which they join. The nerve endings sense pain, touch, temperature and pressure and are Melanocytes are cells found in the deepest layer of the epidermis. There are more nerve produce melanin, which helps protect the body from the sun�s harmful rays. Sweat from the axilla and groin areas (apocrine glands) is more oily in nature and produces a characteristic odour when digested by the skin bacteria. Sebum is an oily substance that keeps the skin moist and acts as a barrier against foreign substances. Hair follicles produce the various hair types that can be found around the body, so can affect a person�s appearance. Hair is also involved in protecting the body from injury and can improve sensation. The thicker reticular dermis contains dense connective tissue, larger Hypodermis blood vessels, elastic fbres and bundles of collagen arranged in layers. It is essential for protection of internal body�s defence against infection structures and also provides insulation. This is important if a diagnosis of urticaria or herpes simplex is being considered. The important question here is the time interval after sun exposure until the rash appears. In solar urticaria, the rash appears within fve minutes of sun exposure and is gone within an hour; in polymorphic light eruption, the rash occurs several hours after sun the diagnosis of skin disease begins with taking a history. If at this stage a diagnosis Ask about irritants on the skin if the patient has hand eczema. Common irritants include detergents, oils and some solutions that the following information is needed to make a correct diagnosis. This is the most important What treatment has been used to date (medical, herbal and over question in the history. While itching is distressing to the patient, it may not help you reach a diagnosis. Severe itch, especially at night, may be caused by scabies (see section 06 for Scabies). Management of pruritus is an essential component of overall management of the skin condition.
Dramamine 50mg on-line. Everything You Need to Know About the Keto Diet.