

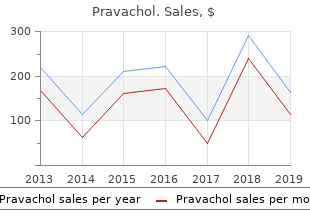
Pravachol
"Purchase pravachol australia, cholesterol and eggs."
By: Denise H. Rhoney, PharmD, FCCP, FCCM
- Ron and Nancy McFarlane Distinguished Professor and Chair, Division of Practice Advancement and Clinical Education, UNC Eshelman School of Pharmacy, Chapel Hill, North Carolina

https://pharmacy.unc.edu/news/directory/drhoney/
Two common types of strabismus are patients with an esotropia cholesterol medication no muscle pain purchase pravachol 20 mg on-line, their eye(s) turned in cholesterol in home grown eggs order pravachol in india, and patients with exotropia cholesterol medication zocor side effects buy discount pravachol on line, their eye(s) turned out high fiber cholesterol lowering foods discount pravachol on line. Patients with an exotropia will have crossed diplopia while patients with an esotropia will have uncrossed diplopia (figure 7). Our visual world comprises of multiple points, hence, the need to develop concepts to deal with the whole visual space. The horopter is the locus of points in space that stimulates corresponding points. All points on this circle should stimulate corresponding points on the retina and lead to single vision, provided that the fixation point lies on the centre of the circle and the eyes rotate about its nodal point (instead of their centre of rotation). The Vieth-Muller circle assumes there is angular symmetry of the corresponding points (figure 8). The circle represents the theoretical locus of points in space that stimulates corresponding retinal points. Instead, the haplopic method determines the inner and outer boundaries of single binocular vision and the horopter is taken as the midline. Haplopic Method the haplopic method (method of the region of singular binocular vision) is based on the primary definition of corresponding points; retinal points which correspond give rise to identical visual directions and, as a consequence, single vision. Therefore the method involves determining the boundaries of single binocular vision (figure 9). Result of the horopter determined by the haplopic method at a viewing distance of 40 cm (Moses R. If the two parts are seen in the same direction then the objects are in that position where they stimulate corresponding points. This is the basis of the Nonius method (method of equating visual directions; figure 10). If there is no depth difference between an object and the fixation point then they stimulate corresponding points. Thus if the subject is asked to arrange a series of objects so that they appear to be in a fronto-parallel plane (ie. The horopter as determined by the apparent fronto-parallel plane method at different distances (25cm, 40cm and 1m). This concept allows for single binocular vision about the point of fixation even when corresponding retinal points are not being stimulated. An image on the retina of one eye can be fused (and seen as single) with a similar image on the retina of the other eye, even though disparity in the retinal image exists. When this is performed, the apparent fronto-parallel plane becomes skewed about the fixation point, with the horopter being nearer on the side of the eye having the increased magnification (figure 12). As long as the magnification difference between the two eyes is not too large, fusion will be maintained although spatial distortions will occur. Aniseikonic symptoms are a common complaint of patients with unequal refractive errors or large astigmatic corrections. If symptoms persist, reducing the magnification difference or reducing the correction are two clinical options. It is possible to appreciate the relative location of objects using one eye (monocular cues). However, it is the lateral displacement of the eyes that provides two slightly different views of the same object (disparate images) and allow acute stereoscopic depth discrimination. Monocular Cues Several strong monocular cues allow relative distance and depth to be judged. Monocular movement parallax Relative Size: Retinal image size allow us to judge distance based on our past and present experience and familiarity with similar objects. Parallel lines converge with increasing distance such as roads, railway lines, electric wires, etc (figure 3). Due to the scattering of blue light in the atmosphere, creating "wall" of blue light, distance objects appear more blue (figure 4). When the scattering of light blurs the outlines of objects, the object is perceived as distant. Because our visual system assumes the light comes from above, a totally different perception is obtained if the image is viewed upside down. Closer objects move "against" the direction of head movement and farther objects move "with" the direction of head movement. Fusion describes the neural process that brings the retinal images in the two eyes to form one single image. When the objects are different, suppression, superimposition or binocular ("retinal") rivalry may occurs. Binocular rivalry describes alternating suppression of the two eyes resulting in alternating perception of the two images. This usually occurs when lines are presented to the two eyes differ in orientation, length or thickness. An example of binocular rivalry occurs when one eye is presented with a horizontal line and the other eye is presented with a vertical line. Binocular rivalry occurs at the intersection of the lines and some suppression also exists (figure 6) Figure 6. Haplopic method of determining the horopter involves locating the region of single binocular vision at a distance of 40cm. Retinal disparity is essential for stereoscopic depth perception as stereoscopic depth perception results from fusion of slightly dissimilar images. Due to the lateral displacement of our eyes, slightly dissimilar retinal images result from the different perception of the same object from each eye. Clinical Tests used to measure Stereopsis There are two groups of clinical tests used to measure stereopsis. Random-dot stereograms were first used by Julesz (1960) to eliminate monocular cues. As there are no contours, depth perception (stereopsis) can only be appreciated when binocular fusion occurs. Global stereopsis is required in random-dot stereogram when the evaluation and correlation of corresponding points and disparate points are needed over a large retinal area. An example of a contour stereotest used in the clinic is the Titmus Fly Stereotest. In the Titmus Fly Stereotest, horizontal disparity is presented via the vectographic technique (Fricke and Siderov, 1997). When tested a 40 cm the fly has a disparity of 3,600 sec of arc; the disparity of the animals range from 400 100 sec of arc and the disparity of the Wirt rings range from 800 40 sec of arc (fig u r e 8). In one of the squares, a circle of these geometric shape is painted on the other side of the perspex. The Randot Stereotest uses modified animals and ring designs with random dot backgrounds to eliminate monocular cues. The Lang Stereotest uses a panographic technique (Fricke and Siderov, 1997) to present disparity, therefore, no filters are required. The working distance and interpupillary distance will need to be taken into consideration when calculating stereoacuity. Patients with disturbed binocular vision or different refractive error in one eye, will perform poorly on depth discrimination tests. The human visual system can detect and discriminate between an incredibly diverse assortment of stimuli that may be chromatic or achromatic, in motion or not, pattered or unpatterned, two-dimensional or three. Remarkably, the neural end-product of visual stimuli impacting upon the retina is, in one sense, always the same. After the complexities of phototransduction, lateral interactions provided by horizontal and amacrine cells, and integration of signals by ganglion cell dendrites only the constantly changing stream of action potentials propogating along ganglion cell axons is left to inform our visual perception. These seemingly identical signals must somehow be processed in the subcortex and cortex to create the full range of visual percepts we experience. How this is achieved is a puzzle that currently occupies the professional lives of thousands of researchers and the basic framework of a solution has only begun to unfold in the last several decades. To achieve an understanding of cortical and subcortical processing we can ask two basic questions about the signals leaving the retina: � What are the discrete anatomical pathways that carry the signal That is, the answers we have so far are incomplete and, in many cases, conflicting.
The spiral muscles wrap around in such a manner that contribute to cholesterol levels mg/dl buy on line pravachol the con traction or �wringing� out of the blood of the heart cholesterol risk ratio purchase 20 mg pravachol with mastercard. Inotropic agents and intra-aortic balloon counterpulsations may also be indicated cholesterol yogurt buy pravachol american express. Clopidogrel (Plavix) may also be used as a substitute or as dual antiplatelet therapy high cholesterol medication over the counter purchase cheap pravachol. Warfarin (Coumadin), a vitamin K antagonist, has shown no benet and may increase bleeding risk. They should be initiated during hospital ization and continued long term (unless contraindicated). Early recognition and management with inotropic therapy, intra-aortic balloon counterpulsation, and surgery can improve outcomes. The contributing factors of a thrombus include inammation of the endocardium and a hypercoagulable state. The presentation is an embolic stroke and symptoms depend on the location of the embolus. Anticoagulation therapy is used to manage the thrombus (heparin followed by warfarin for 3�6 months). Newer hemody namic monitors that are minimally invasive and that use the arterial waveform may also be used to assist with the diagnosis. Inotropes are recommended in hypoperfusion states with or without pulmonary congestion, but may be initiated at a lower dose in cardiogenic shock to limit complications. It may not improve the 30-day survival but it has been shown to improve long-term survival (6-month and 6-year outcome studies). A patient who develops an atrial utter and is hemodynamically compromised requires synchronized electrical cardioversion. The difculty with the ventricular lling may be caused by an incomplete ventricu lar relaxation, increased stiffness, pericardial restraint, or high intrathoracic pressure. The diagnostic �gray area� is between 100 and 500 pg/mL and anything greater than 500 pg/mL is positive. Others, develop a dry, hacking cough that can interfere with activities of daily living. Hypokalemia may adversely affect cardiac conduction and lead to arrhythmias and sudden death. There is a lengthwise separation of the medial layer due to a tear in the intima with intramedial extravasation. Blood ows between the intimal and medial layers creating a double lumen, called a false lumen and a true lumen. Dissection can be acute, present within the rst 14 days of initial injury, or chronic, with presentation longer than 14 days. Shearing forces can also cause further tears, producing exit sites and ow back into the true lumen (Box 1. There is sometimes a �latency� period during which the pain will get better after the initial onset, but then it returns as a �knife-like� severe pain. Another assessment includes assessing pulses in the upper limbs compared to the lower limbs. A signicant pulse decit in the lower extremity should also increase level of suspicion (Box 1. The aortogram can pinpoint the site of intimal tear, the true and false lumen entry site, appearance of dye outside of the aorta, and bulging of aorta. If contrain dicated to use a blocker, the second choice of drugs is nondihydropyridine calcium chan nel-blocking agents, which should be utilized as an alternative for rate control. Surgical intervention is recommended with an aneurysm in the descend ing aorta greater than 5. Other indications for surgery include a saccular aneurysm or postsurgical pseudoaneurysm. Goals of surgery include repair of aorta as well as preven tion of ischemic insult to distal organs. Surgical procedures on aorta can include intimal ap repair, removal of thrombosis and false lumen, replacement of dilated aorta with a graft, repair of aortic root, and replacement of aortic valve. Endovascular repair may also be used in descending aortic dissections through femoral access. Postoperative management includes assessing for signs of coagulopathy and continued reversing of heparin. They may also use other spinal cord perfusion techniques such as proximal aortic pressure maintenance and distal aortic perfusion to optimize spinal cord perfusion (Box 1. Antihypertensive agents used pre operatively may be continued in the postoperative period. Hemodynamic monitoring, prevention of uid overload, correct coagulopathy, and administration of antibiotics to prevent graft infections are components of postoperative management. Manipulation of the catheter during interventional stent placement can break loose debris and become a distal embo lism. The superior and inferior mesen teric arteries may be involved in a descending aortic dissection. Pathophysiology Is pericardial tamponade considered a diastolic or systolic dysfunction Following an injury, blood accumu lates within the pericardial sac, causing a constriction on the heart. The pericardial pressure becomes higher than the ventricular lling pressures, interfering with the ability of the ventri cles to ll with blood (diastolic phase). The amount of blood required to impair lling depends upon the rate of the accumulation of blood and the compliance of the pericardial sac. The presentation of a classical Beck�s triad occurs with an acute cardiac tamponade. It may also detect pericardial uid, thrombus, and collapsing of the ventricular wall during diastole. Passive elevation of the legs may also be used to increase venous return and improve ventricular lling. Pericardiocentesis can also be performed using landmarks or guided by echocardiogram and by placing a drain tube. Pericardotomy can also be performed using a balloon to create the pericardial window. Contusion sever ity ranges from subepicardial to intramural hemorrhage into the intraventricular septum. The severity of the arrhyth mia does not correlate with the severity of the contusion (Box 1. It is also used to identify patients requiring cardiac monitoring and the presence of complications, such as pericardial effusion. Other management issues include hemodynamic stabiliza tion and treatment of associated injuries. Complications Following a blunt chest trauma, a patient develops a new-onset systolic murmur. A rupture (regurgitation) of the mitral valve results in a systolic murmur, whereas a rupture of the aortic valve would cause a diastolic murmur (Box 1. The mitral valve should be closed during systole (systolic murmur) and the aortic valve must close during diastole (diastolic murmur). If the patient survives to the emergency department, he or she will usually have a small tear or a partial-thickness tear of the aorta forming an aneurysm. Pathophysiology A traumatic aortic aneurysm is most likely to be caused by what mechanism of injury The aorta is relatively mobile in the chest and will continue to travel after the sudden deceleration except where it is secured by a ligament. The ligamentum of arteriosum secures the proximal descending thoracic aorta, just distal to the arch (at the level of the isthmus). During the sudden deceleration, this ligament holds the aorta back while the arch of the aorta continues to travel. Other sites of xation include the ascending aorta, the aortic root, and the diaphragmatic hiatus.
Purchase pravachol 20 mg. Cholesterol good - Medical Definition.
This resulted in com the individuals with CoA cholesterol healthy foods cheap 20mg pravachol fast delivery, without resulting in significant parable systolic and mean arterial pressures in Turner change average cholesterol test purchase cheapest pravachol and pravachol. In addition to cholesterol grams chart buy pravachol 10mg lowest price ever cholesterol levels mg/dl cheap pravachol 20mg visa, it would be unethical to investigate a similar group this, 24-h ambulatory diastolic blood pressure correlated of people without treatment, and the fact that these Wen et al. Journal of Cardiovascular Magnetic Resonance (2018) 20:80 Page 11 of 12 women were receiving their usual treatment makes this Ethics approval and consent to participate study a reflection of a real-life outpatient clinic cohort. The study protocol conformed to the ethical guidelines of the Declaration of Helsinki and was approved by the Central Denmark Region Ethical Scientific Committee Conclusion (#2012�500-12) and registered at ClinicalTrials. Adult Turner Syndrome females have impaired aortic Consent for publication wall function of the ascending and descending aorta, �Not applicable� with reduced aortic distensibility among those with Competing interests CoA, and higher central and peripheral night-time dia the authors declare that they have no competing interests. The principal determinant of the abnormal aortic Publisher�sNote wall function was the presence of type 2 diabetes, CoA Springer Nature remains neutral with regard to jurisdictional claims in and age. Measurement of aortic distensibility is a prom published maps and institutional affiliations. Division of Endocrinology, Cincinnati Children�s Hospital gender matched controls. Cardiovascular Imaging Department, Cardio-respiratory Unit, Great lower distensibility at the descending aorta. Each dot represents an individual; blue circles are Turner Syndrome with aortic coarctation and black filled are indicate Turner Received: 28 September 2017 Accepted: 23 October 2018 Syndrome without aortic coarctation. Aortic distensibility in women with Turner Syndrome but no aortic coarctation compared to healthy age and References gender matched controls. Each dot represents an individual; blue diagnostic delay, and mortality in turner syndrome. Mortality Lone Kvist, Eva Schriver and Susanne Sorensen are thanked for their expert in women with turner syndrome in Great Britain: a national cohort study. Aortic Augustinus Foundation, the Toyota Foundation, the Aase og Einar Danielsen valve disease in turner syndrome. Carotid intima-media thickness is increased in turner syndrome: the effects of growth hormone treatment in the turner syndrome. Am J multifactorial pathogenesis depending on age, blood pressure, cholesterol Cardiol. J Clin Endocrinol Carotid intima-media thickness and arterial stiffness and the risk of atrial Metab. Arterial stiffness, pressure and flow pulsatility and brain Segmental aortic stiffness in children and young adults with connective structure and function: the age, gene/environment susceptibility-Reykjavik tissue disorders: relationships with age, aortic size, rate of dilation, and study. Dilation of the ascending aorta in turner syndrome a prospective and meta-analysis. Proximal aortic stiffening in turner patients may be present before wave reflections and survival in end-stage renal failure. Nocturnal Marfan syndrome: cardiovascular physical findings and diagnostic correlates. Cardiac malformations and High pulse pressure is not associated with abnormal activation of the renin hypertension, but not metabolic risk factors, are common in Turner angiotensin-aldosterone system in repaired aortic coarctation. Abnormal aortic arch morphology in turner syndrome patients is a risk Abnormal wave reflections and left ventricular hypertrophy late after factor for hypertension. Relationship between blood pressure parameters and pulse wave velocity in normotensive and 28. Vascular remodeling after "successful" repair of coarctation: impact of aortic 51. Vascular smooth muscle cells Hemodynamic correlates of abnormal aortic root dimension in an adult and arterial stiffening: relevance in development, aging, and disease. Local stiffness of the carotid and femoral artery is associated with incident cardiovascular events and all-cause mortality: the Hoorn study. Aortic stiffness and carotid intima-media thickness: two independent markers of subclinical vascular damage in young adults Interrelationship between non-invasive measurements of atherosclerosis: flow-mediated dilation of brachial artery, carotid intima-media thickness and pulse wave velocity. When placed within the target lesion, the stent graft provides an alternative conduit for blood flow within the patient�s vasculature by excluding the lesion from blood flow and pressure. The stent graft system is composed of 2 main components: the implantable Valiant thoracic stent graft and the disposable Captivia delivery system. The stent graft is preloaded into the delivery system, which is inserted endoluminally via the femoral or iliac artery and tracked through the patient�s vasculature to deliver the stent graft to the target site. Alternatively, it may be used in combination with additional stent graft sections that increase the graft length either distally or proximally to the primary section. All stent graft components are composed of a self-expanding, spring scaffold made from Nitinol wire sewn to a fabric graft with non-resorbable sutures. The metal scaffolding is composed of a series of serpentine springs stacked in a tubular configuration. Radiopaque markers are sewn onto each component of the stent graft to aid in visualization and to facilitate accurate placement. Stent graft components should be oversized to be larger than the measured healthy vessel. Stent Graft Materials Component Material Springs Nitinol wire (55% Nickel, balance Titanium with trace elements) Support Spring Nitinol wire (55% Nickel, balance Titanium with trace elements) Graft Fabric High-density woven mono-filament polyester Sutures Braided polyester Radiopaque Markers Platinum-Iridium wire the Valiant thoracic stent graft with the Captivia delivery system does not contain natural rubber latex; however, during the manufacturing process, it may have incidental contact with latex. Mini Support Spring Note: this and all other product graphics appearing in this manual are not drawn to scale. They are for graphical representation only, and may appear differently under fluoroscopy. The Valiant thoracic stent graft is available in 4 configuration options: FreeFlo Straight (proximal component), Closed Web Straight (distal component), Distal Bare Spring Straight (distal component), and Closed Web Tapered (distal component). Each consists of an 8-peak, fully covered stent and a mini support 4 spring, which prevents the stent graft from infolding during and after deployment. FreeFlo Straight Configuration (Proximal Component) this configuration includes a FreeFlo proximal end and a Closed Web distal end. At the proximal end, an 8 peak bare stent extends past the covered stent graft to provide additional fixation while maintaining transvessel flow. The FreeFlo Straight configuration stent grafts are available in diameters ranging from 22 mm to 46 mm and covered lengths of approximately 100 mm, 150 mm, and 200 mm. The proximal-end and distal-end diameters of the FreeFlo Straight configuration are constant throughout the covered length of the device. Caution: A FreeFlo end should never be placed inside the graft covered section of another stent graft. Closed Web Straight Configuration (Distal Component) this configuration includes Closed Web proximal and distal ends. The Closed Web Straight configuration stent grafts are available in diameters ranging from 22 mm to 46 mm and covered lengths of approximately 100 mm, 150 mm, and 200 mm. The proximal and distal end diameters of the Closed Web Straight configuration are constant throughout the covered length of the device. Caution: A Closed Web Straight configuration may be implanted as the primary section only when implanting multiple stent grafts in a nontortuous segment of the descending thoracic aorta, using the distal-to-proximal implantation technique. Distal Bare Spring Straight Configuration (Distal Component) this configuration includes a Closed Web proximal end and a Bare Spring distal end. At the distal end, an 8 peak bare stent extends past the covered stent graft to provide additional fixation while allowing for transvessel flow. The Distal Bare Spring Straight configuration stent grafts are available in diameters ranging from 22 mm to 46 mm and a covered length of approximately 100 mm. The proximal and distal end diameters of the Distal Bare Spring Straight configuration are constant throughout the covered length of the device. Caution: A Bare Spring end should never be placed inside the covered section of another stent graft. Closed Web Tapered Configuration (Distal Component) this configuration includes Closed Web proximal and distal ends. The Closed Web Tapered configuration stent grafts are available in proximal end diameters ranging from 26 mm to 46 mm and distal end diameters ranging from 22 mm to 42 mm.
Bilateral exophthalmos oc pulsatility of the proptosis the cause could be a carotid� curs almost always in endocrine exophthalmos cholesterol levels ideal cheap pravachol 20 mg with mastercard, but bilateral cavernous fstula or transmitted pulsations from the cranium cholesterol levels explained uk cheap pravachol 20 mg visa, proptosis is seen in the later stages of thrombosis of the as seen with the loss of bone in neurofbromatosis cholesterol joint pain purchase cheap pravachol on-line. Proptosis cavernous sinus cholesterol glucose ratio buy pravachol canada, empyema of the accessory sinuses of the that increases on the Valsalva manoeuvre or on bending nose, symmetrical orbital tumours (lymphoma, pseudoleu forwards is probably caused by a vascular lesion such as kaemia), and as a result of diminished orbital volume in varicosities of the orbital veins. Optic atrophy from pressure on Computerized Tomography in Orbital Lesions the nerve occurs in the other forms. Fat, a tissue of low density, in the intraconal space acts as a natural contrast medium. This also provides the clinician with information the bones of the foor of the orbit are fractured and soft as to the anatomical extent of any space-occupying lesion, tissues herniate into the maxillary sinus. It may also be the especially when it also involves the paranasal sinuses, or result of a resolved orbital cellulitis, which is followed by extends into the cranium. Metastasis to the orbit, scanner for orbital diagnosis lies in its ability to take scans. It allows the be made to determine whether the invasion of the orbit is ophthalmologist to determine the type of tissue affected, the secondary or whether the growth is primarily orbital. This is important in both the diagnosis and in planning therapy for such patients. It is capable of imaging soft tissues, not only within the orbit but within the globe itself, Plain X-rays allowing better tissue diagnosis of an orbital lesion. Plain X-rays of the orbit highlight bony disorders which Computerized tomographic scans are preferred for contribute to a proptosis or other orbital disease. Posteroanterior views of the if the presence of a magnetic foreign body is suspected. In the rectus muscle cone and for in blow-out fractures of the orbit as it delineates the apex of the orbit, a high proportion of obstruction in the intra foor of the orbit and the sinuses. Special views are required conal course of the superior ophthalmic vein is due to an in for imaging of the optic foramen and superior orbital fs fammatory process. Other patients requiring carotid angiogra phy are those with a vascular tumour in the orbit where it is important to identify the feeding vessel before surgery. Pre-septal cellulitis is treated with appropriate oral Periostitis antibiotics, depending on the source of the infection, and this is rare but particularly affects the orbital margin. The resolution is most often due to injuries, extension of infammation from generally quick and complete. In traumatic In orbital cellulitis there is extensive swelling of the lids cases, it is the margin that is naturally most affected, but with chemosis (Fig. The eye is proptosed and its a traumatic element is often an exciting cause in the mobility impaired with resulting diplopia. Pain is severe, other cases, so that in them also the margin suffers most increased by movement of the eye or pressure. Vision may be Periostitis of the deeper parts of the orbit causes less reduced owing to retrobulbar neuritis or compression of the defnite signs. If the apex of the orbit is implicated, various ocular the extraocular muscles, orbital fat and congested veins. If suppuration supervenes, the abscess is opened and of extension to the meninges and brain as purulent menin any carious bone removed. In diabetics a particularly fulminant infection with be necessary and should not be too delayed. Treatment: After taking blood samples for culture, in travenous treatment with broad-spectrum antibiotics and Orbital Cellulitis this is a purulent infammation of the cellular tissue of the orbit. It is due most frequently to extension of infammation from the neighbouring parts, especially the nasal sinuses; other less common causes are deep injuries, especially those with a retained foreign body, septic operations, poste rior extension of suppurative infections of the eyelids or the eyeball such as panophthalmitis, facial erysipelas, or metastases in pyaemia. There are two recognized types of orbital cellulitis with differing presentations, therapy and prognosis. Pre-septal A orbital cellulitis involves structures anterior to the orbital septum that is largely the lids. Orbital cellulitis is a term reserved for infections behind the orbital septum, which may or may not spill over to the lids. Pre-septal cellulitis commonly presents as a swelling of the lids, with erythema and chemosis (Fig. The presence of a localized abscess may necessitate through the middle meningeal veins and the veins of Vesa prolonged therapy or drainage of the pus. The anastomo Thrombosis of the Cavernous Sinus ses of the ophthalmic veins with the frontal and angular veins opens up a communication with the face. Labyrin Sources of Infection thine veins opening into the inferior petrosal sinus afford a this may be due to extension of thrombosis from various communication with the middle ear. The supe the sinus in communication with the subcutaneous tissues rior and inferior ophthalmic veins enter it from the front behind the ear, through the lateral sinus and superior petro sal sinus, and is of great diagnostic importance, since a swelling behind the ear may decide the question of throm Superior Tributary bosis in each direction along these sinuses. The sinus of ophthalmic vein one side communicates with that of the other by two Tributary (or sometimes three) transverse sinuses, which surround Cavernous sinus the pituitary body. Infection may occur via the orbital veins, as in erysipe las, septic lesions of the face, orbital cellulitis, and infective conditions of the mouth, pharynx, ear, nose and accessory Superior petrosal sinus sinuses, or as a metastasis in infectious diseases or septic conditions. On more than one occasion bilateral blindness Inferior petrosal sinus has resulted from an event as simple as the injudicious squeezing of a furuncle on the upper lip. Symptoms and Signs Lateral the patient presents with almost the same symptoms and sinus signs as in orbital cellulitis, but with systemic features such as fever, headache and an altered sensorium. Thrombosis of the cavernous sinus is accompanied by rigors, vomiting and severe cerebral symptoms. The frst sign is often paralysis of cases may require cyclophosphamide in addition to steroids the opposite lateral rectus, and this should be carefully and radiation. Tolosa�Hunt Syndrome There is severe supraorbital pain owing to involvement of the branches of the ophthalmic division of the trigeminal One of the lesions of the orbital apex, this syndrome is char nerve, and paresis of the ocular motor nerves. In the later acterized by painful, acute ophthalmoplegia, with or without stages the eye is immobile, the pupil dilated, and the cornea involvement of the optic nerve and ophthalmic division of anaesthetic. Proptosis occurs in nearly all cases, but is of the trigeminal nerve and it responds promptly to steroid late onset in those of otitic origin. Tolosa described a case in which a mass of It is commonly stated that the retinal veins are greatly granulation material was found around the carotid artery in engorged, but in many cases this is not true. When this the cavernous sinus; this syndrome is now referred to as the occurs it is usually accompanied by pronounced disc swell Tolosa�Hunt syndrome. The patient should be fully investi ing and both signs indicate extensive implication of the gated to eliminate diagnoses such as infraclinoid aneurysm, orbital veins and tissues. Typical papilloedema is common carotid�cavernous fstula, pituitary tumour, meningioma est in otitic cases and indicates meningitis or cerebral and orbital tumour. Simultaneous thrombosis of both cavern 24�48 hours, as well as any signs of compression. Other ous sinuses, with proptosis and disc swelling, occurs in lesions may be responsive to steroids but neither is the diseases of the sphenoid sinuses. If, in addition, there is remission complete nor does it occur so rapidly after the oedema in the mastoid region behind the ear the diagnosis onset of treatment. The Tolosa�Hunt syndrome is not a is certain, as it is due to thrombosis of the emissary vein. This should be managed together by both Parasitic Infestations of the Orbit neurologists and ophthalmologists. Trichinosis this is an infestation of the striated muscles by the larva Idiopathic Orbital Infammatory Disease of the nematode Trichinella spiralis. The encysted larvae Idiopathic orbital infammatory disease, also known as non are ingested in undercooked pork and develop in the intes specifc orbital infammatory disease or pseudotumour, is of tine into mature adults. It produces proptosis due to a non most common in areas where raw or undercooked pork, neoplastic mass in the orbit. Eggs develop and hatch when all other causes of infammatory masses have been in the female nematode and the larvae enter the general discounted. It can occur at any age but is commonest between Nausea, diarrhoea, vomiting, fatigue, fever and ab 40 and 60 years and slightly commoner in men. Headache, fever with chills, cough, eye swelling, joint and It is usually unilateral but occasionally bilateral. There is pain on movement of insertion, which is useful in differentiating this from the eyes. In such cases radiotherapy is often effective in this stage, though albendazole appears to be marginally eliminating the disease permanently. A trial of Chapter | 30 Diseases of the Orbit 491 albendazole is thus justifed in severe or prolonged infec tions.