

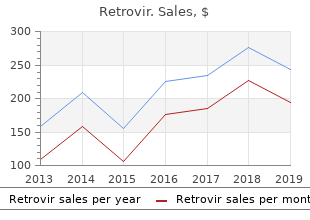
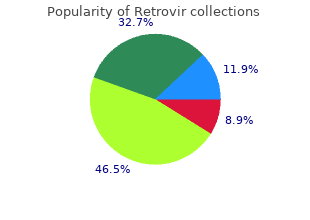
Retrovir
"Order retrovir 100mg mastercard, medications known to cause pill-induced esophagitis."
By: Paul Reynolds, PharmD, BCPS
- Critical Care Pharmacy Specialist, University of Colorado Hospital
- Clinical Assistant Professor, Department of Clinical Pharmacy, Skaggs School of Pharmacy and Pharmaceutical Sciences, University of Colorado, Aurora, Colorado

http://www.ucdenver.edu/academics/colleges/pharmacy/Departments/ClinicalPharmacy/DOCPFaculty/Q-Z/Pages/Paul-Reynolds,-PharmD.aspx
History from others on scene treatment xerosis order retrovir on line, including seizures or shaking medications kosher for passover generic retrovir 100mg visa, presence of pulse/breathing (if noted) symptoms 0f a mini stroke buy 300mg retrovir with visa, duration of the event treatment action group quality 100mg retrovir, events that lead to the resolution of the event c. Patients suffering syncope due to arrhythmia may suffer recurrent arrhythmia and should therefore be placed on a cardiac monitor 2. Geriatric patients suffering falls from standing may sustain significant injury and should be diligently screened for trauma � go to General Trauma Management guideline Notes/Educational Pearls Key Considerations 1. Consideration of potential causes, ongoing monitoring of vitals and cardiac rhythm as well as detailed exam and history are essential pieces of information to pass onto hospital providers. The emergency department approach to syncope: evidence-based guidelines and prediction rules. Atypical or unusual symptoms are more common in women, the elderly and diabetic patients. Assess the patient�s cardiac rhythm treat pulseless rhythms, tachycardia, or symptomatic bradycardia [see Cardiovascular and Resuscitation guidelines] 3. Administer aspirin; chewable, non-enteric-coated aspirin preferred (162 to 325 mg) 6. Examples are: sildenafil (Viagra, Revatio), vardenafil (Levitra, Staxyn), tadalafil (Cialis, Adcirca) which are used for erectile dysfunction and pulmonary hypertension. Also avoid use in patients receiving intravenous epoprostenol (Flolan) or treporstenil (Remodulin) which is used for pulmonary hypertension. It is especially important for the treating physician to be informed if the patient is taking beta-blockers, calcium channel blockers, clonidine, digoxin, blood thinners (anticoagulants), and medications for the treatment of erectile dysfunction or pulmonary hypertension. Toxin exposure (beta-blocker, calcium channel blocker, organophosphates, digoxin). See additional inclusion criteria, below, for pediatric patients Exclusion Criteria No recommendations Patient Management Assessment, Treatment, and Interventions 1. Transcutaneous Pacing If pacing is performed, consider sedation or pain control 2. Consider the following additional therapies if bradycardia and symptoms or hemodynamic instability continue: i. Epinephrine may be used for bradycardia and poor perfusion unresponsive to ventilation and oxygenation. It is reasonable to administer atropine for bradycardia caused by increased vagal tone or cholinergic drug toxicity Patient Safety Considerations If pacing is performed, consider sedation or pain control Notes/Educational Pearls Key Considerations 1. If medication overdose is considered, refer to appropriate guideline in the Toxins and Environmental section 4. Bradycardia should be managed via the least invasive manner possible, escalating care as needed a. Third-degree heart block or the denervated heart (as in cardiac transplant) may not respond to atropine and in these cases, proceed quickly to chronotropic agents (such as epinephrine or dopamine), or transcutaneous pacing b. Although dopamine is often recommended for the treatment of symptomatic bradycardia, recent research suggests that patients in cardiogenic or septic shock treated with norepinephrine have a lower mortality rate compared to those treated with dopamine 10. Frequency that weight or length-based estimate are documented in kilograms 32 o Hypoglycemia-01: Treatment administered for hypoglycemia. The efficacy of atropine in the treatment of hemodynamically unstable bradycardia and atrioventricular block: prehospital and emergency department considerations. You have confirmed the pump has stopped and troubleshooting efforts to restart it have failed, and ii. The patient is unresponsive and has no detectable signs of life Notes/Educational Pearls 1. Automatic non-invasive cuff blood pressures may be difficult to obtain due to the narrow pulse pressure created by the continuous flow pump 3. The patient�s travel bag should accompany him/her at all times with back-up controller and spare batteries 7. In-hospital cardiopulmonary arrests in patients with left ventricular assist devices. Inclusion Criteria Heart rate greater than 100 bpm in adults or relative tachycardia in pediatric patients Exclusion Criteria Sinus tachycardia Patient Management Assessment, Treatments, and Interventions i. Consider the following additional therapies if tachycardia and symptoms or hemodynamic instability continue: i. Irregular Narrow Complex Tachycardia � Stable (atrial fibrillation, atrial flutter, multifocal atrial tachycardia) 1. Administration of amiodarone, if needed, should follow procainamide in patients with Wolff�Parkinson�White syndrome viii. As it is difficult to ascertain onset of rhythm, risk of stroke needs to be considered prior to cardioversion 3. A wide-complex irregular rhythm should be considered pre-excited atrial fibrillation; extreme care must be taken in these patients a. Wolff Parkinson-White Syndrome, Lown-Ganong-Levine Syndrome) because these drugs may cause a paradoxical increase in the ventricular response c. Patients who receive metoprolol and diltiazem are at significant risk for hypotension and bradycardia 3. Intravenous lidocaine versus intravenous amiodarone (in a new aqueous formulation) for incessant ventricular tachycardia. Impact of a practice guideline for patients with atrial fibrillation on medical resource utilization and costs. Dysconjugate gaze, forced or crossed gaze (if patient is unable to voluntarily respond to exam, makes no discernible effort to respond, or is unresponsive) 4. Use a validated prehospital stroke scale that may include, but is not limited to: a. If the patient was last seen normal prior to bedtime the night before, this is the time to be documented. Revision Date September 8, 2017 45 General Medical Abdominal Pain Aliases None Patient Care Goals 1. Identify life-threatening causes of abdominal pain Patient Presentation Inclusion Criteria Abdominal pain or discomfort related to a non-traumatic cause Exclusion Criteria 1. Obtain vital signs including pulse, respiratory rate, pulse oximetry, and blood pressure 4. Right lower quadrant tenderness noted during palpation of the left lower quadrant (positive Rovsing�s sign) iii. Peri-umbilical or diffuse abdominal tenderness with palpation or �jiggling� of the abdomen/pelvis iv. Reassess vital signs and response to therapeutic interventions throughout transport Patient Safety Considerations None recommended Notes/Educational Pearls Key Considerations 1. Consider transport to a trauma center if aortic aneurysm is suspected 47 Pertinent Assessment Findings 1. Revision Date September 8, 2017 48 Abuse and Maltreatment Aliases Maltreatment of vulnerable populations Definitions 1. Abuse/Maltreatment: Any act or series of acts of commission or omission by a caregiver or person in a position of power over the patient that results in harm, potential for harm, or threat of harm to a patient 2. Recognize any act or series of acts of commission or omission by a caregiver or person in a position of power over the patient that results in harm, potential for harm, or threat of harm to a patient 2. Take appropriate steps to protect the safety of the responders as well as bystanders 3. Clues to abuse or maltreatment can vary with age group of the patient and type of abuse 2. Leave further intervention to law enforcement personnel Inclusion/Exclusion Criteria Absolute inclusion/exclusion criteria are not possible in this area. Rather, clues consistent with different types of abuse/maltreatment should be sought: 1. Potential clues to abuse/maltreatment from caregivers or general environment: 49 a. Information provided by caregivers or patient that is not consistent with injury patterns. Inadequate safety precautions or facilities where the patient lives and/or evidence of security measures that appear to confine the patient inappropriately 2. Potential clues to abuse or maltreatment that can be obtained from the patient: a. Inability to communicate due to developmental age, language and/or cultural barrier b. Report concerns about potential abuse/maltreatment to law enforcement immediately, in accordance with state law, about: a. Document findings by describing what you see and not ascribing possible causes.
Amplification of the red blood cell precursors is under the control of the hormone erythropoietin 897 treatment plant rd 300mg retrovir fast delivery, which is released by the kidney medicine 48 12 order cheapest retrovir and retrovir. The availabilities of intracellular iron and oxygen also regulate the rate of heme synthesis medications jamaica order retrovir with visa. While this isoform is the rate limiting step in red cell heme sythesis symptoms nausea discount retrovir 300 mg, it is not regulated by feedback inhibition from 3 heme. In red cell precursors the requirement for heme synthesis is generally constant for the production of hemoglobin. Iron is a reactive transition metal that is normally present in the body complexed with proteins that limit its chemical reactivity. Iron content within the body is controlled only at the level of iron absorption through the duodenal enterocyte. Small amounts of iron (1 � 2 mg per day) are lost with skin and bleeding, but this is not a regulated process. Most iron available for use in the body is generated by macrophages that recycle iron from red cells. Dietary ferric (Fe iron in the duodenal lumen is converted to ferrous (Fe), absorbed by the duodenal enterocyte and subsequently transported to the blood. Iron is transported in the blood as two atoms of ferric iron bound to transferrin. Transferrin is internalized in heme-producing cells after binding to a surface transferrin receptor. Transferrin ferric iron is converted to ferrous iron within the endosome mitochondrion. Hemosiderin is a form of Ferritin complexed to additional iron that accumulates in the body as a result of iron overload. Iron metabolism is an area of intense investigation, and our understanding is dramatically expanding. Within the last year the central roles of Hepcidin and Ferroportin have been 4 proposed. Ferroportin is the only known protein known to be involved in exporting iron from cells (macrophages, enterocytes, etc. Hepcidin causes the internalization and degradation of Ferroportin; shutting off the egress of iron from the cell. It goes up in inflammatory states, decreasing the amount of iron available for heme synthesis. It is therefore responsible for the Anemia of Inflammation (Anemia of Chronic Disease). Dysregulation of the Hepcidin � Ferroportin interaction is the most likely final pathway for the known forms of Hemochromatosis. Hemojuvelin, a protein in the hepcidin pathway, was identified by identifying a molecular basis for juvenile hemochromatosis. Hemochromatosis is a very common condition in people of northern European extraction. Pattern of porphyrin excretion and clinical manifestations depends on which enzyme affected 4. The molecular basis of the observed �low penetrance� is in the process of being elucidated a. May be erythropoietic, hepatic or mixed depending on main site of synthesis / accumulation 8. Acute Attacks in the �Neurovisceral Porphyrias� are clinically indistinguishable b. Decreased levels of albumin, or drugs that interfere with this binding can allow toxic, unbound bilirubin to leak into the tissues. Conjugated bilirubin is actively transported into the bile canaliculi, and eventually into the bile ducts (with some storage in the gall bladder). Conjugated bilirubin in the bile is released into the intestines, where the bacterial flora converts it to urobilinogen (which is colorless) and then to stercobilin (which gives the brown color to feces 7. Most urobilinogen diffuses from the intestine into the blood supply, where it is delivered to the kidney. Unconjugated bilirubin, which is less soluble and reacts more slowly, is called indirect bilirubin. Indirect bilirubin is usually measured by subtracting the direct bilirubin from total bilirubin (measured by the van den Bergh reaction done in methanol, which solubilizes both forms of bilirubin). Hemolysis causes an elevation of indirect bilirubin because the amount of bilirubin produced exceeds the liver�s conjugating capacity. Obstruction of the bile duct causes backup and elevation of direct bilirubin in the plasma. Jaundice is the symptom which is observed when there is accumulation of bilirubin in the skin and sclera. Kernicterus is toxic bilirubin encephalopathy that is observed in neonates with high levels of unbound bilirubin. All neonates have a tendency toward elevated bilirubin levels because bilirubin glucuronyl transferase is low at birth. Hyperbilirubinemia in the neonate can be treated with blue fluorescent light phototherapy which converts bilirubin to water soluble isomers. Crigler-Najar syndrome is the genetic disease caused by deficiency of bilirubin glucuronyl transferase. Child Development, Child Mental Health and Community Paediatrics 41 Joanne Philpot and Ruth Charlton 3. Acro Background centric chromosomes (13, 14, 15, 21, 22) have the Within the nucleus of somatic cells there are 22 centromere at one end and only a q arm. Selection of the active X chromosome is some complement of 46 chromosomes is known as usually random and each inactivated X chromo diploid. Genomes with only a single copy of every some can be seen as a Barr body on microscopy. Three copies of a single chromosome in diploid daughter cells with nuclear chromosomes a cell are referred to as trisomy, whereas a single which are genetically identical both to each other copy is monosomy. In males the onset of meiosis and spermato ing just one member (homologue) of each chromo genesis is at puberty. The reduction in life but the oocytes remain suspended before the chromosome number occurs during meiosis I and is rst cell division until just before ovulation. Meiosis 278 Genetics Translocations � Webbed or short neck � Low hairline � Reciprocal � exchange of genetic material � Shield chest with widely spaced nipples between non-homologous chromosomes � Cubitus valgus (wide carrying angle) � Robertsonian � fusion of two acrocentric � Cardiovascular abnormalities (particularly aortic chromosomes at their centromeres. These patients There is also commonly an increased risk of mis show little phenotypic abnormality but tend to be of carriage and of reduced fertility. Although intelligence is typically re duced compared with siblings it usually falls within Carriers of a robertsonian translocation involving normal or low�normal limits. However, mild devel chromosome 21 are at increased risk of having opmental and behavioural dif culties are more offspring with translocation Down syndrome. Fertility is normal but the incidence of female and male (14;21) translocation carriers the early menopause is increased. Phenotypic cation carriers can also have offspring with normal abnormalities are rare prepubertally other than a chromosomes or offspring who are balanced trans tendency to tall stature. The testes are small and associated with azoospermia, testosterone production is around 1. Female distribu tion of fat and hair and a high-pitched voice may this affects 1 in 2500 live-born girls but it is a occur but are not typical. Patients reduced compared with siblings but usually falls are usually of normal intelligence. Mild develop streak ovaries that result in failure of menstruation, mental and behavioural problems are more com low oestrogen with high gonadotrophins and infer mon. If puberty is achieved, the uterus is usually normal and pregnancy is possible with the this affects 1 in 1000 live-born boys. In hood with failure of the pubertal growth spurt is telligence is usually within normal limits but there is typical. Final height can be increased by early an increased incidence of behavioural abnormal treatment with growth hormone.
Ironically treatment 30th october buy cheap retrovir online, that will include a return to medicine 02 retrovir 100mg plant medi cines as our primary healing agents for infectious diseases treatment hypothyroidism purchase retrovir 300 mg online. Some of my ancestors symptoms concussion buy discount retrovir, powerful political physicians, actively worked to destroy the W estern tradition of herbal medicines, feeling that they were the outmoded and tragic remnants of a superstitious past. They felt that science would ofer the answers, all the answers, 304 305 What the Future Holds that through science we could defeat all disease organisms on this planet. It is fascinating to me that in the midst of the failure of that utopian and very psychological projection the plants are returning once again to help us in our lives and with our diseases. W e, here a few hundred thousand years (or perhaps a million or two if you take into account earlier expressions of Homo spp. It is no accident, I suspect, that the Cherokee peoples have repeated a legend for generations to their chil dren, a legend that tells of the time plants were asked by the animals and insects (whom the humans had harmed by their lack of aware ness) to turn on humans and give them diseases (just as the animals and insects were doing). A new para digm of healing is emerging, one partly based in the older healing sys tems of the human species (including technological medicine) but one that also contains elements never known before. W e are all going to need each other�s help, you know, and we might as well start now. They are not distinct from the earth, the sun and moon, and the other heavenly bodies. It is therefore absurd to approach the subject of health piecemeal with a departmentalized band of specialists. A medical doctor uninterested in nutrition, in agriculture, in the wholesomeness of mind and spirit is as absurd as a farmer who is uninterested in health. And though it takes time, as your knowledge increases, as you learn how to tend to your illnesses and those of your family, the sense of helplessness that so many of us have experienced when we become ill, often ingrained since birth, begins to dissipate. W e have been trained to place our health in the hands of outside specialists who, very often, know neither ourselves nor our families, not the fabric of our lives nor the communities in which we live. They have no understanding of, and often no interest in, the complexity in which we live and from which our illnesses emerge. But for most of us, those specialists are the only place we know to go when we are ill, uncertain, and afraid, to seek help � for ourselves or our loved ones. All of us live, all the time, in the midst of a living phar macy that covers the surface of this planet. Once you know that, once you have been healed by the plants in that living pharmacy, often of something that physicians said could not be healed, things are never the same again. You begin to break the cycle of dependence on which the health care system depends. Taking back control over personal health and healing is one of the greatest forms of personal empowerment that I know. It does take time and efort, this kind of learning, but the learning goes quickly. It is a truly frightening moment, that moment of decision, when trust is extended in that way, for, before it occurs, there is no way to experientially know what the outcome will be. M ost people on this planet, though, people who do not live in the W estern, industrialized nations, make that deci sion every day of their lives. Trusting the healing capacities of the plants is not a new experience to the human species. The next step is learning how to turn the plants you are learning about into medicines for yourself and your family. It isn�t that hard � people all over the globe have been doing it for a hundred thousand years. It is condensed from a much larger exploration in the second edition of my book Herbal Antibiotics. The main forms of herbal medicines for internal use are: � Water extracts (infusions and decoctions) � Alcohol extracts (tinctures) � Percolations (water or alcohol) � Fluid extracts � Syrups/oxymels/electuaries � Glycerites � Fermentations � Vinegars � Fresh juice (stabilized or not) � Powders (plain or encapsulated) � Food � Suppositories/boluses � Douches � Essential oils � Steams � Smokes the main forms of herbal medicines for external use are: � Oil infusions � Salves � Evaporative concentrates � Washes � Liniments � Lotions � Compresses/poultices � Essential oils � Smudges Most of these you can make yourself. In this condensed version, I will primarily look at alcohol and water extractions. So, herbs were placed in liquids � on particular days by the fanatical � and left in there for one cycle of the moon. Though derided as superstition by scientists there is some legitimacy to this kind of thinking. Plants really are stronger when harvested on certain days, the moon does afect the underground aquifers of the Earth, just as it does the oceans (causing the ground to breathe out moisture-laden air), leeches really are useful (surgeons use them regularly now), maggots really do clean gangrenous wounds better than anything else, and. Anyway, the solvent is called the menstruum, herbs are placed in the menstruum, and once there they begin to macerate. M aceration is the soaking of something � usually a plant of some sort � in a solvent until the cell walls begin to break down so the compounds in the herb will leach into the solvent, where they are held in suspension. When you later separate the liquid (containing the medicinal compounds) from the solids, the solids that are left are called the marc. The liquid is called whatever kind of medicine you were making: tincture, infusion, or so on. W ater is considered to be the universal solvent; it works for most things to some extent. Your water, especially, should be well, spring, or rain water � if you can get it. If you use tap water, have a flter on the water line if you are at all able to do so. When you are making extracts, part of what you learn, and develop in your practice, is knowledge of just what kinds of solvents are right for which herbs and in what combinations. The goal is to get as many of the medicinal compounds as possible into the extractive medium. Each herb is diferent and needs diferent combinations of water and alcohol � that is, a diferent formula for preparation. Some need oils to extract the active constituents (Artemisia annua is an example of this; artemisinin is more easily soluble in fats than in either alcohol or water). This is why pharmacists are still called �chemists� in England and the drugstores there the �chemist�s shops. I doubt there is a medicinal pharma cist in practice anywhere in the world who can prepare a tincture of Colchicum ofcinale and determine, exactly, the amount of colchicine in it � as all pharmacists could do in 1920. In becoming an herbal medicine maker, you are learning how to be a practical dispensing pharmacist. Part of what that means is 310 311 A Brief Look at Herbal Medicine Making discovering how to best prepare the herbs and with which solvents. A brief description follows; my book Herbal Antibiotics includes an herbal formulary that will give you the ratio of alcohol and water for several hundred plant tinctures. Water extractions the two most common forms of water extractions are infusions and decoctions. When making medicine, however, you are usually working with what would formally be called an infu sion. Infusions are stronger than teas since the herbs sit, or infuse, in the water for a much longer period. An infusion is made by immersing an herb in either cold or hot (not boiling) water for an extended time. The weakness of infusions, cold or hot, is that they do not keep well; they tend to spoil very quickly. Infusions, unless you stabilize them with something like alcohol, need to be used shortly after you make them. Their strength is that nearly everyone has access to enough water to make them without resorting to the expense of buying alcohol. Although these guidelines use short timelines for hot infusions, I often make my infusions at night just before bed and let them infuse overnight. M ost hot infusions are consumed, confusingly, not hot but warm or at room temperature; the infusion periods are too long for the water to 312 313 Water Extractions stay hot. Hot infusion, in this sense, is a description of the extraction process, not of its temperature when used. Some herbs, however, are best consumed while still hot, often these are diaphoretics that stimulate sweating. Yarrow, if being used to stimulate sweating to help break a fever, is best consumed hot (steeped 15 minutes, covered). To prepare a hot infusion, bring water to a boil, then pour it over the herb in the following manner: For leaves: 1 ounce per quart of water, let steep 4 hours, tightly covered. If you are using fresh leaves, cut them fnely with scissors or chop them as fnely as pos sible with a sharp knife.

Cavitary disease may occur symptoms 13dpo purchase generic retrovir canada, and while most such lesions will resolve radiographically medications for depression 300mg retrovir sale, a subset may become chronic medicine 93 5298 buy retrovir 100mg without a prescription. More commonly symptoms quivering lips generic retrovir 100mg with visa, computed tomography will allow identification of nodular or cavitary disease and will determine the extent of mediastinal involvement. Eosinophilia may be seen in peripheral blood or in cerebrospinal fluid specimens during active or convalescent disease states. These radiographic and laboratory findings, although suggestive of disease, are less sensitive and specific than complement fixation. The headaches are described as pounding, with nausea and vomiting, but no phonophobia or photophobia. She reports that her weight has increased by more than 20 lbs since her visit 1 year ago. On physical examination, the girl�s blood pressure is 102/78 mm Hg and her heart rate is 92 beats/min. Papilledema may be seen with increased intracranial pressure, so of the choices, this is the most likely finding in this girl. Pseudotumor cerebri is a condition in which there is increased intracranial pressure but no intracranial mass, hydrocephalus, or other structural abnormality. Medications such as isotretinoin or doxycycline can cause pseudotumor cerebri as well. Symptoms of pseudotumor cerebri include headache, nausea, vomiting, transient visual obscurations (the entire visual field briefly turns gray, as in the girl in the vignette), tinnitus, and headache that worsens with bending over. Performing the fundoscopic examination in a darkened room makes it much easier to see papilledema. In patients with new-onset headaches, clinicians should always assess for evidence of increased intracranial pressure. None of the other choices listed are associated with increased intracranial pressure. Symptoms include slowly progressive blurry vision, not transient visual obscurations as described for the girl in the vignette. It can be seen with injury to the brainstem or cerebellum, and sometimes as a medication side effect. It is not a typical finding in increased intracranial pressure, unless the increased pressure is due to a tumor or stroke affecting the brainstem or cerebellum. Orbital bruits, heard on auscultation with the stethoscope bell over the eye, are associated with vascular abnormalities such as carotid stenosis, arteriovenous fistula, or carotid cavernous fistula. The girl in the vignette does not have symptoms of an intracranial vascular abnormality, so this is not the best choice. Ptosis and pupillary miosis are 2 of the 3 findings in Horner syndrome, the third is anhidrosis. Horner syndrome can occur from disruption of the sympathetic pathway that innervates the eye, anywhere along its course from the brain, neck, chest and up to the orbit. It is not a sign of pseudotumor cerebri, and so would not be an expected finding in the girl in the vignette. Physical examination findings among children and adolescents with obesity: an evidence-based review. The boy has been having major behavioral problems with inattention and aggression toward adults and peers, both at home and school. He has been otherwise well, with only minor illnesses, and his physical examination findings are normal. The foster parents ask you about the child�s risk for future behavioral and physical health problems as a consequence of his maltreatment. In recent years, a growing body of evidence indicates that chronic or repeated stress, such as occurs with abuse/neglect, can result in physiologic and anatomic changes. The concept of �toxic stress� proposes that strong, frequent, or prolonged activation of stress response systems (the hypothalamic-pituitary-adrenal and sympathetic-adrenomedullary systems) without the buffering presence of a nurturing or supportive adult disrupts brain, neuroendocrine, and immune development during developmentally sensitive periods. This leads to anatomic changes and physiologic dysregulation that may be lifelong, and is the basis for the chronic stress-related physical and behavioral health problems seen in adults who were abused as children. Human and animal studies show that individuals who encounter adverse events such as abuse during early development have lower overall brain volumes with architectural and size differences in the amygdala (necessary for emotional regulation), hippocampus (necessary for encoding and retrieving memory), and prefrontal cortex (the seat of executive function). In addition to central nervous system effects, there is evidence of immune hyperreactivity among children and adults with a history of abuse and neglect, a likely contributor to the observed increased incidence of asthma and elevated inflammatory markers (eg, C-reactive protein). Adults who were abused as children have higher prevalences of cardiovascular disease, lung and liver disease, hypertension, diabetes mellitus, and obesity compared with the general population. Available evidence, derived largely from retrospective studies, suggests a wide range of behavioral health consequences for children experiencing abuse and neglect, ranging from normal functioning to adverse outcomes such as school failure, unemployment, poverty, incarceration, mood disorders, post-traumatic stress syndrome, interpersonal problems, substance abuse, borderline personality disorder, somatization, psychosis, and dissociative identity disorder. The role of nature versus nurture has long been debated regarding children with these outcomes. A better framework in which to consider early childhood adversity, including abuse and neglect, has been proposed by Shonkoff et al as an �ecobiodevelopmental� approach, which considers multiple factors, including physiological adaptations and disruptions, epigenetics, anatomic development, and children�s social and physical environment. Prevention is the ideal approach to reduce the long-term effects of child abuse and neglect; however, this is not always feasible. A supportive home, with fair and consistent discipline, is recommended for all children. However, for those who experienced early childhood adversity, this approach alone is often not sufficient. Routine discipline that is effective for a child without a history of toxic stress may be perceived as a stress-inducing threat to a previously abused child, and may cause escalation of the behavior rather than extinction. Cognitive behavioral therapy that addresses safety skills, stress management, and emotion regulation, as well as the formulation of an organized and accurate trauma narrative, has proved effective for symptom reduction in other trauma-related situations. The clinical presentation of the child in this vignette with bloody diarrhea and a history of consumption of unpasteurized cow milk is consistent with gastroenteritis caused by Campylobacter species. Campylobacter jejuni and Campylobacter coli colonize the gastrointestinal tracts of chickens, turkeys, and other farm animals and are present in their environment; rates of Campylobacter colonization in chickens are up to 80%. Transmission of Campylobacter infection occurs by ingestion of unpasteurized milk, undercooked poultry products, or contaminated water or by contact with infected animals or humans. Outbreaks of Campylobacter infection in schools following ingestion of unpasteurized milk have been reported in the United States. Person-to-person spread of Campylobacter infection has resulted in outbreaks of gastroenteritis in day care centers and hospital nurseries. Campylobacter species are gram-negative, spiral, motile, non�spore-forming bacilli. The most commonly implicated diarrhea-causing Campylobacter species are C jejuni and C coli, whereas C fetus can cause intestinal infection and severe systemic infection. The Centers for Disease Control and Prevention funds the Foodborne Diseases Active Surveillance Network at 10 United States sites, and this network reported an incidence of 13. In resource-rich countries, cases of Campylobacter enteritis peak during the summer and early fall. Infection with Campylobacter species typically manifests as an acute gastrointestinal illness with fever, diarrhea, and crampy abdominal pain. The diarrhea may be watery but can become mucoid with frank blood mimicking inflammatory bowel disease. In neonates and young infants, the illness may be characterized by bloody diarrhea without fever. The illness is often self-limited with clinical recovery noted within 1 week without antibiotic therapy. Complicated disease (eg, extraintestinal infections, bacteremia) may occur following infection with C fetus or other species in immunosuppressed individuals; in addition, a prolonged course and relapses may occur in immunosuppressed individuals. Immune mediated complications including Guillain-Barre syndrome (and variant Miller Fisher syndrome), reactive arthritis, Reiter syndrome, myopericarditis, and erythema nodosum may occur following Campylobacter infection. Campylobacter species grow slowly, and isolation may be problematic in routine stool cultures. Campylobacter jejuni and C coli can be isolated from stool specimens by using selective media and a microaerobic environment; these species grow best in 5% to 10% oxygen and at a temperature of 42�C. Non�culture-based methods (such as enzyme immunoassays) are available for rapid diagnosis of C jejuni and C coli, but false-positive results can occur. Recently, more sensitive multiplex polymerase chain reaction assays have been developed to detect Campylobacter species and other common enteric pathogens. Most patients with Campylobacter enteritis will recover with treatment of dehydration and replacement of fluids and electrolytes, without the need for specific antimicrobial therapy.
Cheap 300mg retrovir with mastercard. The SMART Way Of Quitting Smoking.