

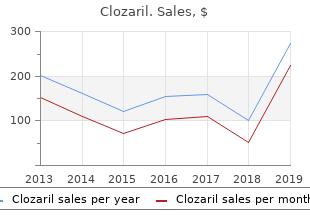
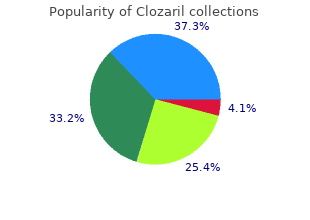
Clozaril
"Discount clozaril online american express, medicine x topol 2015."
By: Paul Reynolds, PharmD, BCPS
- Critical Care Pharmacy Specialist, University of Colorado Hospital
- Clinical Assistant Professor, Department of Clinical Pharmacy, Skaggs School of Pharmacy and Pharmaceutical Sciences, University of Colorado, Aurora, Colorado

http://www.ucdenver.edu/academics/colleges/pharmacy/Departments/ClinicalPharmacy/DOCPFaculty/Q-Z/Pages/Paul-Reynolds,-PharmD.aspx
The medical deci gilancia e da documentacao adequada de cada reaccao medicine gabapentin discount clozaril on line, de sion to medications in spanish cheap 100 mg clozaril visa use a particular drug must consider the risks of pres molde a tentar-se evitar a tempo lesoes causadas por far cribing the drug against the potential benefits for each indi macos medicine river animal hospital clozaril 25 mg fast delivery. There are a great number of potential etiologies for acute A higher incidence rate has been found in patients with pancreatitis keratin intensive treatment cheap 25mg clozaril overnight delivery, one of which is drug-induced pancreatitis. Drug-induced pancreatitis occurs in the general popula the severity of drug-induced pancreatitis is generally tion at a rate of around 1. In a case of acute pancreatitis for which no fatal outcome at least from azathioprine (after renal other reasonable aetiology is present, drug aetiology transplantation) (6), ddI (7), frusemide (8) and hydro should be considered as the possible cause. That is the case with statins, which causal drugs in adult patients are azathioprine, have been recently cited as culprit in isolated cases of mesalazine/sulfasalazine, didanosine (ddI), oestrogens, acute pancreatitis. We present a case of acute pancreati furosemide, hydrochlorothiazide, rifampicin, pentami this in which simvastatin was considered responsible after dine, metronidazole, sulphonamides, tetracyclines and exclusion of other known causes of acute pancreatitis. She denied creas with extension to the left perirenal area, which one habitual or occasional alcohol ingestion and had no pre week later showed peripheral delimitation by radio vious history of biliary lithiasis or abdominal trauma and graphic contrast (Figure 2), densification of the mesen no family history of pancreatitis. There gnosed with hypercholesterolemia: 294 mg/dL (N 150 were no areas of pancreatic necrosis. There was no pleu 225) one year prior to admission, for which simvas ral fluid and no ascites. Biliary and liver pathology were tatin was prescribed and which the patient had been on not demonstrated. She did not report any other disease and also the patient had three Ranson/Imrie criteria of clinical denied taking any other medication. She was in mentioned criteria, the patient could probably expect distress, but eupneic and hydrated. The clinical picture improved after a few days of fasting Heart and lung sounds were normal on auscultation. Meanwhile prophylactic omepra was elicited in the epigastrum, but there was no peri zole and ciprofloxacin were administered. Normalisation of all other blood tests was there were no cutaneous signs or legs oedema. The statin induced pan mortality and yet they remain underrated and misunders creatitis may be a class effect, as there are published tood. By definition an adverse drug reaction is a res case reports of pancreatitis apparently due to several of ponse to a drug which is noxius and unintended, and the statins currently in use: atorvastatin (10), simvastatin which occurs at doses normally used in man for prophy (11), rosuvastatin (12), lovastatin (13), fluvastatin (14) laxis, diagnosis, or treatment of disease or for the modi and pravastatin (15). Assessing statin was related to a second episode of drug-related causal connections between drugs and disease is impor pancreatitis (12). Some authors lance of these aspects requires tools for describing have proposed drug interaction as a trigger mechanism. Other authors the drug or dose reduction), and response to rechallenge have reported cases of pancreatitis occurring in patients (drug readministration). These criteria can be organised taking statins in combination with salycilates (17), to gauge the causal link between a drug and an adverse fenofibrate (18), or gemfibrozil (19). Some patients had been ble/likely grades is that the latter grade does not include using the statin for years before the onset of pancreatitis a rechallenge procedure. Only in 3 cases based on case reports, it is not yet known whether dif (13, 14, 20) had the statin been reintroduced resulting in ferent statins carry different risks (17), or if the reintro recurrence of pancreatitis. The clinical course of statin duction of another statin or the same type of statin pre induced pancreatitis was mild for most of the reported viously associated with another drug, will cause another cases. Meanwhile it is advisable that cated the course of acute pancreatitis and, one of these clinicians do not reintroduce any statin, unless absolute patients developed renal failure (16). We think that it is preferable to re creatitis induced by the combination of lovastatin and commend a constant low fat diet and, if necessary to use gemfibrozil was complicated by pseudocyst formation another type of drug to lower cholesterol or tryglice (19). This is why many of these should be carefully questioned about drugs that may be reports are reported as probable/likely cases of statin responsible for inducing the disease. As the use of statins induced pancreatitis and not as certain cases of statin increases, physicians should consider the diagnosis of induced pancreatitis. The definition of probable/likely drug induced pancreatitis in patients taking these me cases of drug-induced adverse reactions means a clinical dications who then develop abdominal pain not event, including an abnormal laboratory test result, that explained by any other process. If statin induced pancre occurs within a reasonable time frame of the adminis atitis is suspected, probably the drug should probably be tration of the drug, and that is unlikely to be attributed permanently discontinued. In our patient, the aetiology to concurrent disease or other drugs or chemicals, and of acute pancreatitis was attributed to simvastatin, which follows a clinically reasonable response on withdrawal had been prescribed for hyper-cholesterolemia, and (dechallenge). Rechallenge information is not required which the patient has been taking for one year without to fulfill this definition (25). We considered it una A consideration of pathophysiological pathways and dvisable for the patient to restart statin therapy. Three causal associations can help the physician to identify months after her episode of acute pancreatitis, the patient adverse drug reactions in complex clinical scenarios. Physicians should be required to report accurate data In our case, all the other usual causes of acute pancre regarding certain and probable/likely adverse drug reac atitis were ruled out. Adverse dence of gallstone disease and serum values of calcium drug reactions at established usual doses are eight times and of cholesterol and triglycerides were normal at the more frequent than idiosyncratic reactions. Other cau tant is to mention the severity of the event, the probable ses were also excluded by the clinical story and physical causal association between the drug use and the event, examination. In these patients we can consider undertaking a more extensive evaluation for the diagnosis of certain entities Correspondencia: such as occult microlithiasis (bile crystals), sphincter of Oddi dysfunction, pancreas divisum and other congeni Antonio Guilherme Neves Murinello tal abnormalities, pancreatic and ampullary neoplasia, Av Eng Ant Azevedo Coutinho, Lt 8 r/c dto genetic causes and autoimmune pancreatitis (26). Aliment with the occurrence of only one isolated and fairly mild Pharmacol & Therap 1996; 10: 23-8. Drug induced acute pan approach, rather than for example to proceed with an creatitis: incidence and severity. Clinical Safety Data Management: Definitions and Standards for enterol 1987; 82: 865-70. Comparison of the algorithms used to eva bly induced by atorvastatin and rosuvastatin. A method for estimating the probability of adverse drug reac concomitant Gilbert syndrome. We start by explaining the embryological and ontogenetic development of the pancreas and describe the basic anatomical characteristics of the mature gland, i. These form the foundation necessary to understand the mechanisms of acinar and ductal cell secretion and their regulation, which are covered in the middle part, with an emphasis on the ionic part of the pancreatic juice. In the last part, we focus on the enzymatic part of the pancreatic juice and its role in digestion of all main groups of energy-rich nutrients, i. Two main sources of additional information will help the reader grasp the main concepts in pancreas physiology:fguressummarize and combine various concepts encountered in the main text, and clinical boxes contain examples of how a given piece of knowledge can be relevant to understand some diseases. Keywords: pancreas, exocrine, development, embryology, anatomy, vascularization, innervation, physiology, pathophysiology, acinar, ductal, cell, molecular, mechanism, regulation, digestion, secretion, nutrient 1. Introduction the main aim of this review of pancreas physiology is to facilitate the understanding of other chapters of this book. It is divided into three main sections that deal with the development and the functional anatomy of the pancreas, with the two-compartment model of exocrine pancreas � 2017 the Author(s). This chapter is distributed under the terms of the Creative Commons � 2017 the Author(s). This chapter is distributed under the terms of the Creative CommonsAttribution License creativecommons. Together, these topics shall provide a solid ground to understand etiopathophysi ology of the most common pancreatic diseases, their symptoms and crucial clinical character istics, as well as some key diagnostic and therapeutic principles. Functional anatomy of the pancreas this chapter is a brief review of human pancreas development and anatomy, with a special emphasis on the exocrine pancreas from both a physiological and a clinical point of view. In other words, this chapter presents developmental and structural basis to understanding pancreas physiology, its blood and lymphatic vasculature, innervation and the integrative regulation of its function, as well as the clinical symptoms and paterns of spreading in cases of malignancy. Embryological and ontogenetic development of the pancreas All parenchymal cell types of the pancreas (acinar, ductal and endocrine cells) are derived from primitive endodermal cells of the foregut [1, 2]. In humans, between the 26 and 28 day ofth th gestation, two endodermal diverticula evaginate from the duodenum, thus forming the dorsal and the ventral pancreatic anlage [3�6]. The dorsal pancreatic bud lies in the dorsal mesentery opposite and above the liver bud. The ventral pancreatic bud develops in the ventral mesentery below the liver bud and connects with the bile duct. During further development, both the ventral bud and the bile duct rotate clockwise, as viewed in the craniocaudal direction, until they reach the dorsal pancreatic bud. The ventral pancreas gives rise to the ventral or lower part of the head of the pancreas that involves also the processus uncinatus, whereas the dorsal pancreas gives rise to the rest of the future pancreas, i.
Differentiate irritant diaper dermatitis from candidal and bacterial infections 6 treatment croup discount clozaril 50 mg otc. Differentiate erythema multiforme minor from erythema multiforme major (Stevens-Johnson syndrome) b medicine wheel clozaril 50 mg visa. Recognize life-threatening complications of erythema multiforme major (Stevens Johnson syndrome) medications via peg tube clozaril 50 mg with amex. Differentiate between erythema multiforme major (Stevens-Johnson syndrome) and other exfoliative dermatoses i treatment models 100mg clozaril overnight delivery. Recognize signs and symptoms of drug reactions in the skin, including urticaria, fixed drug eruptions, and photodermatitis c. Differentiate between drug reactions in the skin and common dermatoses and exanthems 8. Distinguish among various dermatoses associated with toxin-producing staphylococci, including staphylococcal scalded skin syndrome, bullous impetigo 9. Recognize and interpret relevant laboratory studies for superficial fungal infections of the skin d. Recognize and interpret relevant laboratory and imaging studies for herpes simplex virus d. Differentiate the etiology by age and understand the pathophysiology of hypoglycemia b. Recognize and interpret relevant laboratory and imaging studies for adrenal hyperplasia d. Recognize and interpret relevant laboratory and imaging studies for diabetes insipidus d. Know the etiology and understand the pathophysiology of hypoparathyroidism and hyperparathyroidism 2. Recognize and interpret relevant laboratory and imaging studies for hypothyroidism d. Recognize how to differentiate rectal prolapse from more serious conditions (eg, intussusception) 4. Know the etiology and understand the pathophysiology of antibiotic-associated enterocolitis b. Differentiate by age the epidemiology and incidence of inflammatory bowel disease b. Know causes of fulminant hepatic failure, including drugs, storage diseases, and autoimmune disorders b. Recognize and interpret relevant laboratory and imaging studies for biliary tract disease d. Recognize and interpret relevant laboratory and imaging studies for pancreatitis d. Recognize and interpret relevant laboratory and imaging studies for gastroesophageal reflux d. Recognize and interpret relevant laboratory and imaging studies for sickle hemoglobin disorders d. Recognize and differentiate by age acute complications of sickle hemoglobin disorders. Know the etiology and understand the pathophysiology of thalassemia major and other hemoglobinopathies b. Recognize and differentiate by age signs and symptoms of neutropenia and neutrophil dysfunction b. Know the etiology and understand the pathophysiology of idiopathic thrombocytopenic purpura b. Recognize signs and symptoms and life-threatening complications of idiopathic thrombocytopenic purpura c. Recognize and interpret relevant laboratory studies for inherited disorders of coagulation. Recognize the signs and symptoms of emergency complications of aplastic and hypoplastic anemias 7. Plan the management of emergency complications of aplastic and hypoplastic anemias 11. Recognize complications of blood products transfusions, eg, infectious, hemodynamic d. Differentiate by age the etiology and understand the pathophysiology of occult bacteremia 2. Recognize and interpret relevant laboratory, imaging, and monitoring studies for sepsis 4. Differentiate by age the etiology and understand the pathophysiology of non-cervical lymphadenitis 2. Recognize and interpret relevant laboratory and imaging studies for non-cervical lymphadenitis 4. Differentiate by age the etiology and understand the pathophysiology of bacterial meningitis 2. Recognize and interpret relevant laboratory and imaging studies for encephalitis 4. Differentiate by age the etiology and understand the pathophysiology of brain abscess, subdural and epidural abscesses, and empyema 2. Recognize life-threatening complications of brain abscess, subdural and epidural abscesses, and empyema 5. Differentiate by age the etiology and understand the pathophysiology of otitis media 2. Differentiate by age the etiology and understand the pathophysiology of mastoiditis 2. Differentiate by age the etiology and understand the pathophysiology of sinusitis 2. Know the etiology and understand the pathophysiology of peritonsillar abscesses 2. Recognize and interpret relevant laboratory and imaging studies for peritonsillar abscesses 4. Recognize and interpret relevant laboratory and imaging studies for retropharyngeal, parapharyngeal, and other deep space head and neck infections 4. Plan management of acute retropharyngeal, pharyngeal, parapharyngeal, and other deep space head and neck infections k. Recognize and interpret relevant laboratory and imaging studies for bacterial pneumonia 4. Recognize signs and symptoms of nonbacterial pneumonia, eg, viral, mycoplasmal, chlamydial, fungal 3. Recognize and interpret relevant laboratory and imaging studies for bronchiolitis 4. Recognize and interpret relevant laboratory and imaging studies for tuberculosis 4. Differentiate by age the etiology and understand the pathophysiology of viral gastroenteritis 2. Differentiate by age the etiology of parasitic and fungal gastrointestinal infections 2. Recognize and interpret relevant laboratory and imaging studies for parasitic and fungal gastrointestinal infections 4. Recognize life-threatening complications of parasitic and fungal gastrointestinal infections 5. Know the etiology and understand the pathophysiology of bloodborne viral hepatitis b. Recognize and interpret relevant laboratory and imaging studies for bloodborne viral hepatitis. Differentiate by age the etiology and understand the pathophysiology of skin and soft tissue infections 2. Recognize the occurrence of osteomyelitis following puncture wounds of the foot 4. Differentiate by age the etiology and understand the pathophysiology of urinary infections b. Know the etiology and understand the pathophysiology of Rocky Mountain spotted fever 2. Recognize and interpret relevant laboratory and imaging studies for Rocky Mountain spotted fever 4. Recognize signs and symptoms of other tickborne diseases (eg, tularemia, relapsing fever) 2.
Nearly half of the events within 24 hours of the procedure an unmonitored setting symptoms quitting weed purchase clozaril with paypal. A Neuromuscular disorders Current respiratory infection history should be obtained to treatment tmj buy clozaril 25 mg line delineate the nature of the murmur medications qd buy generic clozaril 100 mg on line. In most cases medicine in ancient egypt order 100 mg clozaril free shipping, the parents will report that the murmur was detected From Clinical practice guideline: diagnosis and management of childhood obstructive previously by the child�s pediatrician and determined to be an sleep apnea syndrome. Anatomic nasal obstruction have moderate sleep apnea unless one or more of the signs of d. Tonsils nearly touching or touching in the midline (kissing tonsils) symptoms above is severely abnormal. History of apparent airway obstruction during sleep (two or more of observer, child regularly falls asleep within minutes after being left the following are present; if patient sleep is not observed by another unstimulated without another explanation), in which cases patients person, then only one of the following needs to be present) should be treated as though they have severe sleep apnea. Observed pauses in breathing during sleep (Review the polysomnogram for evidence of nocturnal desaturations d. Awakened from sleep with choking sensation <85%, which increases sensitivity to opioids). Frequent arousal from sleep sleep laboratories differ in their criteria for detecting episodes of f. Intermittent vocalizations during sleep apnea and hypoxemia, the Task Force recommends that the sleep g. Child sleeps in unusual positions severity is not indicated, it may be determined by using the following j. Child is often difficult to arouse at usual awakening time Modified from Practice guidelines for the perioperative management of patients with obstructive sleep apnea: an updated report by the American Society of Anesthesiologists Task Force on Perioperative Management of Patients with Obstructive Sleep Apnea. Type of surgery and anesthesia Moss and Adams Heart Disease in Infants, Children, and Adolescents Including the Superficial surgery under local or peripheral nerve block 0 Fetus and Young Adult. Requirement for Postoperative Opioids: Point Score 0�3 Frequent respiratory tract infections (a result of compression of airways Opioid requirement by plethoric vessels leading to stasis of secretions and atelectasis) None 0 Central cyanosis (involving warm mucous membranes: tongue and Low-dose oral opioids (tonsillectomy) 1 buccal mucosa) or poor capillary refill High-dose oral opioids, parenteral or neuraxial opioids 3 Absent or abnormal peripheral pulses D. However, if the murmur is harsh and diffcult to aNote: this table has been modified for children. This example has not been clinically validated, and such 452 a scoring system is simply meant to provide guidance. If the misdiagnosis; the only certain means to exclude a structural defect within planned surgery is of an urgent nature, every effort should be the heart is with an echocardiogram. Reduction of the fever should not cardiology have been established in a joint project with the include administration of aspirin, because aspirin may interfere American College of Cardiology, the American Society of Echo with platelet function and is associated with Reye syndrome. It is rapidly absorbed when administered orally, produc disease and a benign family history is rated as a �rarely appropriate� ing adequate blood concentrations within several minutes. In general, nonpathologic murmurs occur during systole contrast, rectal administration requires at least 60 minutes to and are soft and nonradiating with normal feel to peripheral achieve a signifcant blood concentration. Postoperative apnea in and undergoing hernia repair, although there was at least one former preterm infants after inguinal herniorrhaphy: a combined analysis. Although the majority of former preterm infants in our microanalysis were anesthetized with halothane, 467 apnea that an existing fever predisposes to a malignant hyperthermic has been reported with all anesthetics, including sevofurane, desfurane, reaction. The incidence of subglottic stenosis is this therapy should be continued postoperatively. However, the pharmacokinetics of caffeine an analysis of eight published prospective papers from four change dramaticaly with age: in older infants. This analysis determined that (1) apnea was strongly may contribute to the development of postoperative apnea. There was significant institution-to-institution Postconception age (weeks) variability. Note that there is rapid matura with the highest rate of apnea were also those that used continuous recording tion of the ability to excrete caffeine and that by 60 weeks of postconceptional devices. One should not expect a single dose in former preterm infants after inguinal herniorrhaphy: a combined analysis. Preoperative Evaluation, Premedication, and Induction of Anesthesia 65 Central also associated with a signifcant failure rate (20% in some studies) nervous system and the need for multiple attempts to achieve accurate placement of the needle, 474, 491, 492 although in experienced hands, the success Sepsis Congenital rate for placing a spinal block was 97. Apnea Since our microanalysis in 1995, 467 much has changed: new inhalation agents have replaced halothane, artifcial surfactant Metabolic Others has rescued many infants, and improved respiratory strategies have reduced barotrauma-induced chronic pulmonary disease. Those that anesthesiologists are most often preterm infants should not be anesthetized as outpatients even when a involved with are of metabolic, pharmacologic, or respiratory origins. With respect to full-term neonates, three reports have described �Pharmacologic� infants who developed apnea after apparently uneventful general Central sedation 493�495 anesthesias. It is Fatigue important to identify the composition and rate of administration Apnea of these fuids so that potential intraoperative complications can be avoided. It is best not to puncture the capacity and thereby increasing the propensity to develop hypox line for administering medications or changing fuid. Do not discontinue the glucose-containing solution, because Regional anesthesia has been used to reduce the risk of the relative hyperinsulinemic state could induce hypoglycemia, postoperative apnea. An infusion device should be used at all times so that the rate of (~6% in former preterm infants). In addition, since all of the infants in the to avoid intraoperative hypoglycemia. Perioperative and intraoperative monitoring of glucose, potas compared with the 1995 study, in which all were anesthetized sium, sodium, and calcium, as well as acid-base status, is with halothane, the use of a more modern anesthetic agent did important for long procedures. Preoperative assessment should include a thorough postoperative or intraoperative apnea. Several disease associated with prolonged mechanical ventilation and protocols have been advocated for glycemic control in diabetics. A more detailed discussion of the using gestational age, oxygen dependence at 36 weeks and post perioperative management of the child with diabetes is presented conceptual age, total duration of oxygen supplementation, and in Chapter 27. These infants suffer from hypoxemia, reported, and children appeared to recover from anesthesia at a hypercarbia, abnormal functional airway growth, tracheomalacia, usual rate. None of the patients were noted to have increased bronchomalacia, subglottic stenosis, increased pulmonary vascular seizure activity postoperatively. Pulmonary function also describe successful administration of general anesthesia to abnormalities, including a reduced functional residual capacity, children following ketogenic diets without adverse events. For longer procedures, preparation should focus on optimizing oxygenation, reducing serum pH or bicarbonate levels should be checked preoperatively airway hyperactivity, and correcting electrolyte abnormalities and at routine intervals intraoperatively. Serum pH and bicarbonate monitoring paid to fuid balance and avoiding excessive hydration. Adequate should be continued postoperatively until the patient restarts a expiratory time to avoid excessive positive-pressure ventilation is full ketogenic diet. Long-term (>2 hours) propofol infusions, which impair using a smaller than expected tracheal tube. The possibility of fatty acid oxidation, are not recommended in patients following pulmonary hypertension and right ventricular dysfunction should ketogenic diets as fatal propofol infusion syndrome has been be considered and, when indicated, evaluated via electrocardiogram described, but brief infusion should not be problematic (see also and echocardiography. It is important to obtain of the antiseizure medications, medication schedule, and possible a detailed family history, and if the child has not been previously interactions between these medications and anesthetic drugs. If a sickle test is stress of surgery and anesthesia may lower the seizure threshold positive and the surgery is elective, then surgery should be and cause a seizure. Seizure medications should be continued postponed pending hemoglobin electrophoresis to more carefully until the time of elective surgery. It must be empha manifestations of the seizure is useful to be able to diagnose sized that the status of hydration and oxygenation is critical for potential seizures postoperatively. Meticulous attention to detail to ensure stable and postoperative management of anticonvulsant blood con cardiovascular and ventilatory status establishes adequate oxygen centrations may also ensure proper therapeutic effect (see also ation to prevent sickling. Further recommendations regarding manage ratio of fat to carbohydrate and protein. The exact mechanism ment of these children, including indications for preoperative by which the diet works is unclear. All patients were in ketosis, as demonstrated by preoperative serum hydroxybutyrate levels. Death or neurologic injury after tonsil sevofurane, nitrous oxide, propofol, thiopental, and ketamine.
Clozaril 100mg for sale. Gallstones (cholelithiasis) - causes symptoms diagnosis treatment & pathology.