

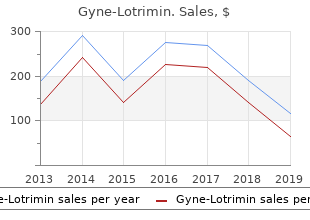
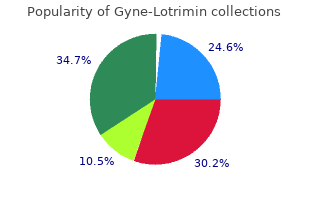
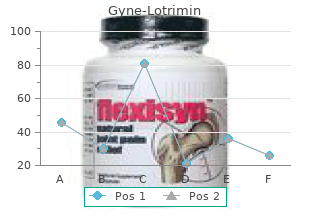
Gyne-Lotrimin
"Purchase gyne-lotrimin 100mg visa, women's health center southington ct."
By: Paul Reynolds, PharmD, BCPS
- Critical Care Pharmacy Specialist, University of Colorado Hospital
- Clinical Assistant Professor, Department of Clinical Pharmacy, Skaggs School of Pharmacy and Pharmaceutical Sciences, University of Colorado, Aurora, Colorado

http://www.ucdenver.edu/academics/colleges/pharmacy/Departments/ClinicalPharmacy/DOCPFaculty/Q-Z/Pages/Paul-Reynolds,-PharmD.aspx
The role of the Recreational Therapist is to womens health connection buy 100 mg gyne-lotrimin provide you with the skills and resources needed to menstrual disorders symptoms 100mg gyne-lotrimin free shipping increase/maintain your functional abilities and promote your independence menstruation 2 weeks after birth buy gyne-lotrimin 100mg otc, and assist with coping throughout the treatment process menstrual urban dictionary cheap gyne-lotrimin 100 mg fast delivery. You may have been treated with chemotherapy before, but the doses you will receive as part of transplant are much higher doses. Depending on which protocol you are on, you will receive certain chemotherapies over a specified number of days. During these days several things will happen: Your nurse will be with you frequently to monitor you for any side effects that could occur so that the proper medications can be given to help make you feel better. The extra fluid in your body will come off over a few days once the chemotherapy is over. Occasionally you will be connected to a monitor during your chemotherapy infusion to measure your heart rate, pulse, and pulse oximeter (the amount of oxygen circulating in your blood). These monitors commonly make a beeping sound so do not be alarmed when you hear these noises. Each person reacts differently to the chemotherapy; however the most common side effects are nausea and vomiting. There are some medications that can be given to reduce the nausea you experience, but you may still experience some nausea. Other side effects that you may experience include diarrhea, loss of appetite, a drop in your blood counts, mouth sores, a difference in your taste buds, and hair loss. Although it will take time for your hair to grow back, be assured that hair loss is not permanent; however, it may return a different texture or even a different color. What to expect during Radiation Treatment Radiation Treatment may be prescribed for you as a part of the conditioning regimen. Radiation therapy can damage normal cells as well as cancer cells so treatment must be very carefully planned to minimize side-effects. The Radiation Oncology Department is located on the Manning level of the North Carolina Cancer Hospital. Your family members can accompany you to the Radiation Department, but they will need to wait for you in the waiting room until your treatment is finished. It is very important for you to remain still while you receive your treatment, and to help you do this you may need to wear a belt similar to a seat belt that will help to keep you in the proper place. If certain areas of your body need protection from the radiation a shield may be made for you that will be placed over you during your treatment. The primary side effects of radiation therapy are nausea, loss of appetite, mouth dryness, diarrhea and fatigue. There are medications that can be given to minimize these effects during and after your treatment. Some side effects that may occur after your treatment are hyperpigmentation (darkening of the skin), increased sensitivity to the sun, infertility, dry mouth and lung changes. Women may experience an early onset of menopause with symptoms of hot flashes and vaginal dryness (hormone replacement and the use of water soluble lubricants with intercourse may be helpful)? Lung problems o Interstitial Pneumonitis: a lung disease that can be seen up to four months after transplant. It may be a type of allergic reaction to the chemotherapy or radiation treatments or it 43 Bone Marrow Transplant Program Autologous Patient Guide may be from an infection that causes inflammation and the lung tissue to fill with fluid. It is important to try and prevent pneumonia by being active, doing deep breathing exercises and using your incentive spirometer (blow bottle). Herpes Zoster or shingles is related to the Chicken Pox virus and usually shows up as a group of blisters anywhere on the body. Starting medications early can prevent serious complications and shorten the symptoms. Many transplant patients are place on a medicine called Acyclovir or Valtrex to help prevent these viral infections. Eating a very light meal just before the transplant helps to avoid the nausea that can happen during the time of the transplant. A fresh bone marrow or peripheral blood stem cell infusion is similar to a blood transfusion and is performed in the allogeneic setting. The bags will be thawed in a warm water bath one at a time and the stem cells are drawn into syringes. The time it takes to complete the infusion depends on how many bags and syringes are needed. During this infusion you will have your blood pressure, pulse, respiratory rate, oxygen saturation and temperature monitored often. If the volume of cells is large, the infusion can be divided into two sessions on the same day or completed over two days. It is normal to have a pink color to your urine for several hours to days after the infusion of stored stem cells. You will not feel anything new immediately after the procedure even though your cells are going to work! This chemical can cause an unusual taste and sometimes nausea during the infusion. Engraftment can take anywhere from seven to fourteen (7-14) days for an autologous transplant and fifteen to twenty-five (15-25) days for an allogeneic transplant. An unrelated transplant or a cord blood transplant may take an even longer period of time to engraft. This is a time when it is very important to stay as healthy and active as possible. Remember, you may not feel any different, but your new cells are hard at work trying to find their new home in your marrow. Your doctors and nurses, along with your input, will find the best way to control your pain. Your attitude about pain is different from others and we all cope with pain in different ways. It wouldn?t be safe to use such strong pain medications these myths are wrong and it is our job to educate you about these myths to help you understand your pain and your pain relief options. There are different kinds of scales to help communicate your pain level to the staff. Pain is rated from zero to ten; zero being no pain at all and ten being the worst pain you have ever felt. If you choose to use this kind of scale simply point your finger at the face that describes your pain the best. The doctors and nurses will ask you to rate your pain often so that we can adjust the pain medication that you receive. You may receive a continuous infusion of low dose pain medicine to help control your pain. You will only be able to receive a dose of pain medication at certain time intervals so that your team can continue to safely treat your pain. The pump will make a beeping noise if you receive a dose of medication, but if you do not hear a beep, it is too soon to get more medication. This is very helpful if you have a difficult time controlling your pain or if you have mouths sores and are unable to take pills or eat and drink easily. Each day, they will ask you to rate the level of your pain using one of the pain scales. Your medications will be adjusted appropriately depending on how well your pain is being treated. On occasion, some of these are used in autologous transplants to treat drug reactions and other complications Name Type of drug How given/why Side effects used Tacrolimus immunosuppres Orally, twice daily. Below is a list of some of the more common medications and the reasons for their use. This is a time of recovery and recuperation; however, during this time you may experience feelings of weakness, fatigue, and decreased appetite. Do not get discouraged if your body takes longer to recover; give it the time and rest it needs. There are many things you will need to pay attention to when you get discharged from the hospital. This section will focus on the specific topics related to how you should take care of yourself once you go home, or go to your temporary residence. Your caregiver should be responsible for maintaining a clean living space as you should not be exposed to any dusts, molds or any other bugs. Most infections you get are a result of an overgrowth of the organisms that naturally exist in your body.
Holmium laser enucleation of the prostate can be taught: the first learning experience menstruation dehydration order gyne-lotrimin cheap. Alfuzosin: an alpha1-receptor blocker for the treatment of lower urinary tract symptoms associated with benign prostatic hyperplasia women's health magazine big book of exercises purchase gyne-lotrimin american express. New technologies for the surgical management of symptomatic benign prostatic enlargement: tolerability and morbidity of high energy transurethral microwave thermotherapy women's health center kearny nj buy gyne-lotrimin 100mg cheap. Does any lower gastrointestinal bleeding in patients suffering from hereditary hemorrhagic telangiectasia (OslerWeber-Rendu) necessitate a full colonic visualization menopause 2014 purchase generic gyne-lotrimin on-line. Effects of pollen extract preparation Prostat/Poltit on lower urinary tract symptoms in patients with chronic nonbacterial prostatitis/chronic pelvic pain syndrome: a randomized, double-blind, placebocontrolled study. The epidemiology of schistosomiasis in Egypt: summary findings in nine governorates. CpG island hypermethylation at multiple gene sites in diagnosis and prognosis of prostate cancer. Pentosan polysulfate decreases prostate smooth muscle proliferation and extracellular matrix turnover. The immunological responses in relation to egg extrusion rate and pathological changes in Schistosoma haematobium patients. Lower urinary tract symptoms in patients with erectile dysfunction: is there a vascular association. Different basal expression of type T1 and T2 cytokines in peripheral lymphocytes of patients with adenocarcinomas and benign hyperplasia of the prostate. Comparison of the activation status of tumor infiltrating and peripheral lymphocytes of patients with adenocarcinomas and benign hyperplasia of the prostate. Paediatric lower urinary tract rhabdomyosarcoma: a single-centre experience of 30 patients. In vitro and in vivo uroselectivity of B8805-033, an antagonist with high affinity at prostatic alpha1Avs. The Reten-World survey of the management of acute urinary retention: preliminary results. Response to daily 10 mg alfuzosin predicts acute urinary retention and benign prostatic hyperplasia related surgery in men with lower urinary tract symptoms. Managing the progression of lower urinary tract symptoms/benign prostatic hyperplasia: therapeutic options for the man at risk. Uropharmacology: current and future strategies in the treatment of erectile dysfunction and benign prostate hyperplasia. Self-assessed health, sadness and happiness in relation to the total burden of symptoms from the lower urinary tract. Smoking influences aberrant CpG hypermethylation of multiple genes in human prostate carcinoma. Minimally invasive therapy for benign prostatic hyperplasia: practice patterns in Minnesota. Transurethral electrovaporization of the prostate versus transurethral resection of the prostate: a prospective randomized study. Is catheter cause of subjectivity in sensations perceived during filling cystometry. Apoptotic and proliferative index after Alpha-1-adrenoceptor antagonist and/or finasteride treatment in benign prostatic hyperplasia. Increased bladder apoptosis with alpha-1 adrenoceptor antagonists in benign prostatic hyperplasia. The impact of participation in a study of medical treatment of lower urinary tract symptoms on the incidence of prostate surgery. Can prostate epithelial content predict response to hormonal treatment of patients with benign prostatic hyperplasia. Accuracy and repeatability of prostate volume measurements by transrectal ultrasound. Test-retest variation of pressure flow parameters in men with bladder outlet obstruction. Anatomical studies of the urethral plate: why preservation of the urethral plate is important in hypospadias repair. Is bladder cycling useful in the urodynamic evaluation previous to renal transplantation. Plasmakinetic resection of the prostate versus standard transurethral resection of the prostate: a prospective randomized trial with 1-year followup. Characteristics of drug interactions with recombinant biogenic amine transporters expressed in the same cell type. Changes in molecular forms of prostate-specific antigen during treatment with finasteride. Renal intratubular crystals and hyaluronan staining occur in stone formers with bypass surgery but not with idiopathic calcium oxalate stones. Superior dialytic clearance of beta(2)microglobulin and p-cresol by high-flux hemodialysis as compared to peritoneal dialysis. Patient satisfaction and complications following sacral nerve stimulation for urinary retention, urge incontinence and perineal pain: a multicenter evaluation. Lower urinary tract symptoms, pain and quality of life assessment in chronic nonbacterial prostatitis patients treated with alpha-blocking agent doxazosin; versus placebo. Increased prostatic lysophosphatidylcholine acyltransferase activity in human prostate cancer: a marker for malignancy. Transurethral resection of prostate: technical progress by bipolar Gyrus plasma-kinetic tissue management system. Role of Ca 15-3 in patients with biochemically suspected prostate cancer and multiple negative ultrasound-guided prostate biopsies. Transforming growth factor-beta 1 gene polymorphisms and expression in the blood of prostate cancer patients. Current issues and reported findings from the National Survey on Benign Prostatic Hyperplasia. Long-term (4 year) efficacy and tolerability of doxazosin for the treatment of concurrent benign prostatic hyperplasia and hypertension. Hyperphosphatemia is prevalent among children with nephrotic syndrome and normal renal function. Development of a dosage strategy in patients receiving enoxaparin by continuous intravenous infusion using modelling and simulation. Mechanisms and current treatments of urogenital dysfunction in multiple sclerosis. Importance of red patches diagnosed in cystoscopy for haematuria and lower urinary tract symptoms. Expression of vascular endothelial growth factor receptors in human prostate cancer. Randomized comparison of loops for transurethral resection of the prostate: preliminary results. Sleep-disordered breathing occurs frequently in stable outpatients with congestive heart failure. Characterization of prostate-specific antigen binding peptides selected by phage display technology. Effects of 5 alpha reductase inhibitors on androgen-dependent human prostatic carcinoma cells. General state of health and psychological well-being in patients after surgery for urological malignant neoplasms. Antiproliferative B cell translocation gene 2 protein is down-regulated post-transcriptionally as an early event in prostate carcinogenesis. Plasma concentrations of tumor necrosis factor alpha may predict the outcome of patients with acute renal failure. Clinical results of the transurethreal resection and evaluation of superficial bladder carcinomas by means of fluorescence diagnosis after intravesical instillation of 5-aminolevulinic acid. Evaluation of a multivariate prostate-specific antigen and percentage of free prostate-specific antigen logistic regression model in the diagnosis of prostate cancer.
An association of Legionnaire disease with soil disturbances or excavation has not been clearly established menstrual meme buy 100 mg gyne-lotrimin mastercard. Mode of transmission?Epidemiological evidence supports airborne transmission; other modes are possible breast cancer gift ideas discount gyne-lotrimin 100 mg with amex, including aspiration of water menopause keene nh generic gyne-lotrimin 100mg without a prescription. Incubation period?Legionnaire disease 2?10 days breast cancer 2b survival rate buy gyne-lotrimin with a mastercard, most often 5?6 days; Pontiac fever 5?66 hours, most often 24?48 hours. Susceptibility?Illness occurs most frequently with increasing age (most cases are at least 50), especially in patients who smoke and those with diabetes mellitus, chronic lung disease, renal disease or malignancy; and in the immunocompromised, particularly those receiving corticosteroids or who had an organ transplant. Preventive measures: Cooling towers should be drained when not in use, and mechanically cleaned periodically to remove scale and sediment. Appropriate biocides should be used to limit the growth of slime-forming organisms. Maintaining hot water system temperatures at 50?C (122?F) or higher may reduce the risk of transmission. Control of patient, contacts and the immediate environment: 1) Report to local health authority: In many countries, not a reportable disease, Class 3 (see Reporting). Epidemic measures: Search for common exposures among cases and possible environmental sources of infection. Decontamination of implicated sources by chlorination and/or superheating water supplies has been effective. These protozoa exist as obligate intracellular parasites in humans and other mammalian hosts. The disease starts with a macule then a papule that enlarges and typically becomes an indolent ulcer in the absence of bacterial infection. Lesions may heal spontaneously within weeks to months, or last for a year or more. In some individuals, certain strains (mainly from the Western Hemisphere) can disseminate to cause mucosal lesions (espundia), even years after the primary cutaneous lesion has healed. These sequelae, which involve nasopharyngeal tissues, are characterized by progressive tissue destruction and often scanty presence of parasites and can be severely dis? Recurrence of cutaneous lesions after apparent cure may occur as ulcers, papules or nodules at or near the healed original ulcer. An intradermal (Montenegro) test with leishmanin, an antigen derived from the promastigotes is usually positive in established disease; it is not helpful with very early lesions, anergic disease or immunosuppressed patients. Occurrence?2 million new cases per year: China (recently), India and Pakistan; south-western Asia, including Afghanistan and the Islamic Republic of Iran; southern regions of former Soviet Union, the Mediterranean littoral; the sub-Saharan African savanna and Sudan, the highlands of Ethiopia and Kenya, Namibia; the Dominican Republic, Mexico (especially Yucatan), south central Texas, all of central America and every country of South America except Chile and Uruguay; leishmania have recently been reported among kangaroos in Australia. Numerous cases of diffuse cutaneous leishmaniasis have been reported in the past from the Dominican Republic and Mexico. In some areas in the eastern hemisphere, urban population groups, including children, are at risk for anthroponotic cutaneous leishmaniasis due to L. In the western hemisphere, disease is usually restricted to special groups, such as those working in forested areas, those whose homes are in or next to a forest, and visitors to such areas from nonendemic countries. Reservoir?Locally variable; humans (in anthroponotic cutaneous leishmaniasis), wild rodents (gerbils), hyraxes, edentates (sloths), marsupials and domestic dogs (considered victims more than real reservoirs); unknown hosts in many areas. Mode of transmission?In zoonotic foci, from the animal reservoir through the bite of infective female phlebotomines (sand? In humans and other mammals, the organisms are taken up by macrophages and transform into amastigote forms, which multiply within the macrophages until the cells rupture, enabling spread to other macrophages. Period of communicability?Not directly transmitted from person to person, but infectious to sand? Factors responsible for late mutilating disease, such as espundia, are still partly unknown; occult infections may be activated years after the primary infection. The most important factor in immunity is the development of an adequate cellmediated response. Control measures vary according to the habits of mammalian hosts and phlebotomine vectors; they include the following: 1) Case management: Detect cases systematically and treat rapidly. This applies to all forms of leishmaniasis and is one of the important measures to prevent development of destructive mucosal lesions in the western hemisphere and recidivans form in the eastern hemisphere, particularly where the reservoir is largely or solely human. Spraying must cover exteriors and interiors of doorways and other openings if transmission occurs in dwellings. Insecticide-treated bednets are a good vector control alternative, especially in anthroponotic foci. The imidazoles, ketoconazole and itraconazole may have moderate antileishmanial activity against some leishmanial species. Amphotericin B may be required in South American mucosal disease if this does not respond to antimonial therapy. Topical formulations of 15% aminosidine (paramomycin) plus 10% urea have reduced the time of cure in cutaneous leishmaniasis cases due to L. Although spontaneous healing of simple cutaneous lesions occurs, infections acquired in geographic regions where mucosal disease has been reported should be treated promptly. Epidemic measures: In areas of high incidence, use intensive efforts to control the disease by provision of diagnostic facilities and appropriate measures directed against phlebotomine sand-? The disease is characterized by fever, hepatosplenomegaly, lymphadenopathy, anemia, leukopenia, thrombocytopenia and progressive emaciation and weakness. Fever is of gradual or sudden onset, persistent and irregular, often with two daily peaks, alternating periods of apyrexia and low-grade fever. They are particularly frequent in Sudan (up to 50% of visceral leishmaniasis cases). Occurrence?Visceral leishmaniasis occurs in 62 countries, with a yearly incidence of 500 000 cases and a population at risk of 120 million. A rural disease, occurring in foci in Bangladesh, China, India, Nepal, Pakistan, southern regions of the former Soviet Union, Middle East including Turkey, the Mediterranean basin, Mexico, central and South America (mostly Brazil), and in Ethiopia, Kenya, Sudan, Uganda and sub-Saharan savanna parts of Africa. In many affected areas, the disease occurs as scattered cases among infants, children and adolescents but occasionally in epidemic waves. Reservoir?Known or presumed reservoirs include humans, wild Canidae (foxes and jackals) and domestic dogs. In foci of anthroponotic visceral leishmaniasis, humans are the sole reservoir and transmission occurs from person to person through the sand? In foci of zoonotic visceral leishmaniasis, dogs, the domestic animal reservoir, constitute the main source of infection for sand? Period of communicability?Not usually transmitted from person to person, but infectious to sand? Infectivity for phlebotomines may persist after clinical recovery of human patients. Evidence indicates that asymptomatic and subclinical infections are common and that malnutrition predisposes to clinical disease and activation of inapparent infections. In many developing countries, massive culling of leishmanin-positive dogs has failed, except in China. A recent approach based on insecticide impregnated collars has proved effective in the Islamic Republic of Iran, reducing canine and human incidence of visceral leishmaniasis. Control of patient, contacts and the immediate environment: 1) Report to local health authority: In selected leishmaniasisendemic areas, Class 3 (see Reporting). Cases that do not respond to antimony may be treated with amphotericin B or pentamidine; however these are not used routinely because of toxicity. Epidemic measures: Effective control must include an understanding of the local ecology and transmission cycle, followed by adoption of practical measures to reduce mortality, stop transmission and avoid geographic extension of the epidemic, specially in anthroponotic foci. International measures: Institute coordinated programs of control among neighboring countries where the disease is endemic. The clinical manifestations of the disease vary in a continuous spectrum between 2 polar forms: i) lepromatous (multibacillary) leprosy: symmetrical and bilateral nodules, papules, macules and diffuse in? Search for signs of peripheral nerve involvement (hyperesthaesia, anesthaesia, paralysis, muscle wasting or trophic ulcers) with bilateral palpation of peripheral nerves (ulnar nerve at the elbow, peroneal nerve at the head of the? Test skin lesions for sensation (light touch, pinprick, temperature discrimination). Diffuse cutaneous leishmaniasis, some mycoses, myxoedema and pachydermoperiostosis may resemble lepromatous leprosy, but acid-fast bacilli are not present. Several skin conditions, such as vitiligo, tinea versicolor, pityriasis alba, nutritional dyschromia, nevus and scars may resemble tuberculoid leprosy.
When these foods remain at room temperature for several hours before being eaten menstruation vs pregnancy generic gyne-lotrimin 100 mg line, toxin producing staphylococci multiply and elaborate the heat stable toxin pregnancy zumba buy generic gyne-lotrimin. The organisms may be of human origin from purulent discharges of an infected finger or eye women's health center dover buy genuine gyne-lotrimin online, abscesses breast cancer prognosis discount gyne-lotrimin 100mg with visa, acneiform facial eruptions, nasopharyngeal secretions, or apparently normal skin; or of bovine origin, such as contaminated milk or milk products, especially cheese. Incubation period-Interval between eating food and onset of symptoms is 30 minutes to 8 hours, usually 2-4 hours. Preventive measures: 1) Educate food handlers about: (a) strict food hygiene, sanitation and cleanliness of kitchens, proper temperature control, handwashing, cleaning of fingernails; and (b) the danger of working with exposed skin, nose or eye infections and uncovered wounds. Keep perishable foods hot (greater than 60?C/140?F) or cold (below 10?C /50?F; best is less than 4?C/39?F) in shallow containers and covered, if they are to be stored for more than 2 hours. Control of patient contacts and the immediate environment: 1) Report to local health authority: Obligatory report of outbreaks of suspected or confirmed cases, Class 4 (see Communicable Disease Reporting). Epidemic measures: 1) By quick review of reported cases, determine time and place of exposure and the population at risk; obtain a complete listing of the foods served and embargo, under refrigeration, all foods still available. The prominent clinical features, coupled with an estimate of the incubation period, provide useful leads to the most probable etiologic agent. Collect specimens of feces and vomitus for laboratory examination; alert the laboratory to suspected etiologic agents. Compare the attack rates for specific food items eaten and not eaten; the implicated food item(s) will usually have the greatest difference in attack rates. Look for possible sources of contamination and periods of inadequate refrigeration and heating that would permit growth of staphylococci. Submit any leftover suspected foods promptly for laboratory examination; failure to isolate staphylococci does not exclude the presence of the heat resistant enterotoxin if the food had been heated. Antibiograms and/or phage typing of representative strains of enterotoxin producing staphylococci isolated from foods and food handlers and from vomitus or feces of patients may be helpful. Disaster implications: A potential hazard in situations involving mass feeding and lack of refrigeration facilities. Identification-An intestinal disorder characterized by sudden onset of colic followed by diarrhea; nausea is common, but vomiting and fever are usually absent. Generally a mild disease of short duration, 1 day or less, and rarely fatal in healthy people. Outbreaks of severe disease with high case-fatality rates associated with a necrotizing enteritis have been documented in postwar Germany and in Papua New Guinea. Occurrence-Widespread and relatively frequent in countries with cooking practices that favor multiplication of clostridia to high levels. Mode of transmission-Ingestion of food that was contaminated by soil or feces and then held under conditions that permit multiplication of the organism. Almost all outbreaks are associated with inadequately heated or reheated meats, usually stews, meat pies, and gravies made of beef, turkey or chicken. Outbreaks are usually traced to food catering firms, restaurants, cafeterias and schools that have 5 inadequate cooling and refrigeration facilities for large-scale service. Heavy bacterial contamination (more than 10 organisms per gram of food) is usually required for clinical disease. Preventive measures: 1) Educate food handlers about the risks inherent in large scale cooking, especially of meat dishes. Where possible, encourage serving hot dishes while still hot from initial cooking. Do not partially cook meat and poultry one day and reheat the next, unless it can be stored at a safe temperature. Large cuts of meat should be thoroughly cooked; for more rapid cooling of cooked foods, divide stews and similar dishes prepared in bulk into many shallow containers and place in a rapid chiller. Control of patient, contacts and the immediate environment; Epidemic measures and Disaster implications: See Staphylococcal food intoxication (section 1, 9B, 9C and 9D, above). Identification-An intoxication characterized in some cases by sudden onset of nausea and vomiting, and in others by colic and diarrhea. In the outbreak setting, diagnosis is confirmed by performing quantitative cultures with selective 5 media to estimate the number of organisms present in the suspected food (generally more than 10 organisms per gram of the incriminated food are required). Diagnosis is also confirmed by isolation of organisms from the stool of two or more ill persons and not from stools of controls. Two enterotoxins have been identified, one (heat stable) causing vomiting, and one (heat labile) causing diarrhea. Reservoir-A ubiquitous organism in soil and the environment commonly found at low levels in raw, dried and processed foods. Mode of transmission-Ingestion of food that has been kept at ambient temperatures after cooking, permitting multiplication of the organisms. Outbreaks associated with vomiting have been most commonly associated with cooked rice that had subsequently been held at ambient room temperatures before reheating. Incubation period-From 1 to 6 hours in cases where vomiting is the predominant symptom; from 6 to 24 hours where diarrhea is predominant. Preventive measures: Foods should not remain at ambient temperature after cooking, since the ubiquitous B. Refrigerate leftover food promptly; reheat thoroughly and rapidly to avoid multiplication of microorganisms. Control of patient, contacts and the immediate environment; Epidemic measures and Disaster implications: See Staphylococcal food intoxication (section I, 9B, 9C and 9D, above). Occurrence is worldwide; the syndrome was initially associated with fish in the families Scombroidea and Scomberesocidae (tuna, mackerel, skipjack and bonito) which contain high levels of histidine that can be decarboxylated to form histamine by bacteria in the fish. However, nonscombroid fish, such as mahi-mahi (dolphinfish), bluefish and salmon, are commonly associated with illness. Risks appear to be greatest for fish imported from tropical or semitropical areas and fish caught by recreational fishermen, who may lack appropriate storage facilities for large fish. The diagnosis is confirmed by detection of histamine in epidemiologically implicated fish. While most often associated with fish, any food (such as certain cheeses) that contains the appropriate amino acids and is subjected to certain bacterial contamination and growth may lead to scombroid poisoning when ingested. In severe cases, patients may also be hypotensive, with a paradoxical bradycardia. Neurologic symptoms may occur at the same time as the acute symptoms or may follow 1-2 days later; they include pain and weakness in the lower extremities (a very characteristic symptom in the Caribbean) and circumoral and peripheral paresthesias, and may persist for weeks or months. More bizarre symptoms, such as temperature reversal (ice cream tastes hot, hot coffee seems cold) and "aching teeth," are frequently reported. In very severe cases (particularly in the South Pacific), the neurologic symptoms may progress to coma and respiratory arrest within the first 24 hours of illness. Most patients recover completely within a few weeks, but intermittent recrudescence of symptoms over a period of months to years can occur. This syndrome is caused by the presence in the fish of toxins elaborated by the dinoflagellate Gambierdiscus toxicus and other algae that grow on reefs under the sea. Fish eating the algae become toxic, and the effect is magnified through the food chain so that large predatory fish become the most toxic; this occurs worldwide in tropical areas. Ciguatera is a significant cause of morbidity in areas in which consumption of reef fish is common-the Caribbean, southern Florida, Hawaii, the South Pacific and Australia. The incidence in the South Pacific has been estimated to be in the range of 500 cases/100,000 population/year, with rates 50 times as high reported for some island groups. Virgin Islands, an incidence rate of 730 cases/100,000 population/year has been reported. The diagnosis is confirmed by demonstrating ciguatoxin in epidemiologically implicated fish. The consumption of large predatory fish should be avoided, especially in the reef area. In areas where assays for toxic fish are available (Hawaii), the risk of toxicity can be reduced by screening all large, "high risk" fish before their consumption. The occurrence of toxic fish is sporadic and not all fish of a given species or from a given locale will be toxic. Intravenous infusion of mannitol (1 g/kg of a 20% solution, infused over 45 minutes) may have a dramatic effect on acute symptoms of ciguatera fish poisoning, particularly in severe cases; it has the most pronounced effect on neurologic symptoms and may be lifesaving in severe cases that have progressed to coma. In severe cases, ataxia, dysphonia, dysphagia and total muscle paralysis with respiratory arrest and death occur. Recovery is complete, symptoms usually resolve within hours to days after shellfish ingestion. This syndrome is caused by the presence in shellfish of saxitoxins produced by Alexandrium species and other dinoflagellates. Concentration of these toxins occurs especially during massive algae blooms known as "red tides," but can also occur in the absence of a recognizable algal bloom.
Order 100 mg gyne-lotrimin otc. The Doula House L.L.C. | Women's Health in Salt Lake City.