

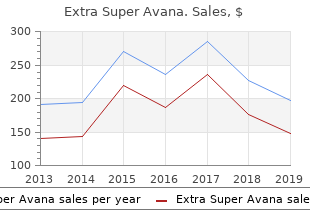
Extra Super Avana
"Purchase extra super avana without a prescription, erectile dysfunction treatment after radical prostatectomy."
By: Denise H. Rhoney, PharmD, FCCP, FCCM
- Ron and Nancy McFarlane Distinguished Professor and Chair, Division of Practice Advancement and Clinical Education, UNC Eshelman School of Pharmacy, Chapel Hill, North Carolina

https://pharmacy.unc.edu/news/directory/drhoney/
Other cancers are much less frequent and make up from a few percent to erectile dysfunction drugs sales buy generic extra super avana 260 mg line a fraction of a percent of cancers among men erectile dysfunction causes natural treatment generic extra super avana 260mg mastercard. Most of the top-10 cancers are connected by an aetiological relation with carcinogenic factors present in tobacco smoke erectile dysfunction treatment needles discount extra super avana online american express. These are erectile dysfunction at the age of 21 buy extra super avana 260mg line, apart from the described lung cancer, pancreatic cancer, urinary bladder cancer and kidney cancer. In the case of oral cavity cancer, pharyngeal cancer, laryngeal cancer and oesophageal cancer, tobacco smoke risk is multiplied by alcohol as an additional risk factor. These cancers are the result of exposure to the sun and are one of the few cancers that show higher incidence levels in women, though the mortality is still higher in men. Incidence of those cancers is steadily growing, and they constitute 7% of all morbidity and mortality. However, some of those cancers are characterised by good treatment results, which lead to their declining mortality. Lyon, France: International Agency for Research on Cancer Available at: http://globocan. Quinn M, Babb P (2002) Patterns and trends in prostate cancer incidence, survival, prevalence and mortality. New England Journal of Medicine 360(13):1320-1328 Verdecchia A, Francisci, S, Brenner H et al. The Lancet Oncology 8(9):784-796 Wilkins D (2006) Tackling the excess incidence of cancer in men: proceedings of the expert symposium. Cancer Res 37:4608-4622 Yamaguchi N, Kakizoe T (2001) Synergistic interaction between Helicobacter pylori gastritis and diet in gastric cancer. Lancet 2:84-94 Zatonski W, Mancuk M, Sulkowska U (2008) Closing the healht gap in the European Union. Male risk taking, the effect of male anti-social behaviour, male work and play activities and the management of mental and emotional conflict are all implicated in the higher rates seen in men. With the exception of sexual violence (for which 90% of victims are women) 72% of interpersonal violence victims and perpetrators are men. Homicide accounting for over 5,500 deaths each year also rises exponentially in young males after the age of 15 and peaks again in the 80 plus age group. In light of the large intercountry variations in mortality rates from injury, it seems prudent that policy lessons and tried and tested preventive programmes established in low mortality countries could be used as a blueprint for good practice initiatives for countries with higher injury mortality rates. If all countries matched those with the lowest mortality rates, half of the lives lost to 256 road traffic injuries and 9 out of 10 of those lost to drowning, poisoning, burns and falls could be saved each year. With men being vastly overrepresented in the injury statistics, such reductions would be particularly significant in reducing mortality and morbidity rates among men. The biggest cause of death within this classification group is accidents accounting for 63% of male deaths (73% female deaths) (Fig. It can be a bodily lesion resulting from acute exposure to energy in amounts that exceed the threshold of physiological tolerance, or it can be an impairment of function resulting from a lack of one or more vital elements (i. The time between exposure to the energy and the appearance of an injury is short (Holder at al. As well as being a major cause of death, accident and injury causes a huge drain on health and other societal resources, resulting in an estimated seven million hospital admissions annually and 60 million medical consultations annually (Bauer & Steiner, 2009). Boys and men are over represented in most fatal and non-fatal accident and injury categories. The burden of accident and injury also varies considerably between and within Member States. The prevalence of accident and injury-related mortality and morbidity is generally higher in Eastern European countries (Sethi et al. This is indicative of an overall pattern of much higher standardised injury death rates in Eastern Europe than Western Europe. The vast majority of injury fatality is attributable to suicide (24%) road traffic accidents (21%) and falls (19%). Injuries affect men and women disproportionately throughout the lifespan with overall risk of injury being approximately twice as high in men (72 injury deaths per 100,000) than in women (35 deaths per 100,000) (ibid). Fatal injury rates (per 100,000) rise sharply up to the age of 15-19, are higher for boys/young men than for girls/young women, and are also much higher in older men than in older women (see Fig. There are also considerable differences between countries in the injury fatality rate for young people. For example, injury accounts for 54% of the total number of adolescent deaths in the Netherlands compared to 76% in Estonia. A) Other causes include: fires, drowning, etc Fatal injury rates also rise dramatically after the age of 70, from 100 to 250 in the age group 80-85 for men (with a corresponding rise from 50 to 150 for women). Among older people (60+) falls (36%) and suicide (28%) are the principal causes of fatal injuries. The rates for road traffic accidents being more than twice as high and suicide more than three times higher for men than for women (Fig. Other causes include: fires, drowning, etc Whilst the proportion of fatalities due to injury amongst older people is relatively small (3% of all deaths), the burden of treatment, rehabilitation and care is enormous. There has been a steady decline in fatalities due to injuries in the past decade (Fig. Developments in homicide figures, road transport and work place accidents are quite favourable, while home and leisure accidents show only a very moderate decline, which most probably is the result of aging societies and the increase in old and frail people, who are frequently affected by falls. This overall decline can be attributable to improvements in injury policy, prevention and legislation, and indirectly through improved surveillance. In the context of the latter, ongoing improvements in the monitoring and recording of injury data is enabling a more informed and targeted approach to injury prevention. Such data is also an important basis for harnessing public support, co-operation between stakeholders and political will, and for monitoring the success and cost-effectiveness of injury-prevention measures (Bauer & Steiner, 2009). Considerable differences exist between countries, with higher rates in Eastern European countries. Although the disparity in road death rates across Europe has decreased since 2001, there is still a fourfold difference between the lowest (Malta) and the highest countries (Lithuania). Indeed, the risk of road traffic injury which is estimated to cause up to 40% of hospital deaths after road traffic accidents could be avoided if appropriate treatment by qualified and trained personnel in appropriately equipped hospitals was available to all victims (Haegi, 2002). The best estimate from the Global Burden of Disease study of the World Health Organization suggests that more than 1 in 3 road traffic fatalities in the European Union are due to alcohol, with males accounting for 15,000 of the 17,000 alcohol related traffic deaths (Anderson & Baumberg, 2006). Alcohol also affects others, including an estimated 10,000 deaths in drink-driving accidents for people other than the drink-driver, and property damage due to drink-driving estimated to be �10bn (ibid). The underreporting of road traffic injuries in police records seems to be particularly high for pedestrians (by a factor of 1. Indeed, more than 40% of vulnerable road user fatalities are recorded among individuals over the age of 60, with the rate being approximately two and half times higher among older men compared to older women (Bauer & Steiner, 2009). Persons over the age of 60 are four times more likely to die when injured by a car compared to younger people (Sklar at al. Not surprisingly, a survey of factors associated with �road risk� in 23 European countries showed that rates of speeding and drink driving were much higher among young men and led to the conclusion that: �When we combine the various findings of this survey we understand that, generally speaking, younger drivers (18-24) engage and admit to more dangerous behaviours. Factors like inexperience, low risk observation, high-risk acceptance, lifestyles, over-estimation of own driving skill, high exposure, can help to explain their engagement in �unsafe� driving behaviour. Such overconfidence in driving ability has been shown to be associated with young men engaging in more frequent reckless driving (Sarker & Andreas, 2004; Farrow & Brissing, 1990); being less likely than young women to consider speeding, drunk driving or distracted driving as dangerous driving behaviours (Sarker & Andreas, 2004), and being less likely to expect a negative consequence to result from such driving behaviour (Farrow & Brissing, 1990). These findings are borne out by a recent Eurobarometer (2010) survey on road safety which found that men were less likely than women to identify as a �major problem� (i) not wearing a seat belt; (ii) driving under the influence of alcohol; (iii) exceeding speed limits; and (iv) driving while talking on a mobile phone (Fig. In Denmark, for example, the rate of accidents involving male drink drivers aged 18�24 is still approximately three times that of 25 to 64 year-olds (Bernhoft et al. Similarly in Ireland, men account for 90% of drink driving offences during the period 2003-2007 (Mongan at al. Luxembourg, Office for Official Publications There are considerable variations between countries, with the highest number of fatal accidents occuring in Italy and Germany (Fig. It is acknowledged that such differences are, to a large extent, the result of methodological differences in surveillance of workplace accidents. Construction, manufacturing and transport, storage and communication account for the highest proportion of fatal accidents (Fig. Approximately two-thirds (68%) of non-fatal accidents occurring among craft and related trade workers, machine operators, 37 or workers employed in an elementary occupation.
This Lisbon Strategy for Growth and Jobs and the Sustainable Development Strategy was based on a prediction of major structural challenges in Europe � globalisation injections for erectile dysfunction cost generic extra super avana 260mg on-line, climate change and the ageing population erectile dysfunction doctors new york buy extra super avana 260 mg on line. The goal of these two initiatives was to erectile dysfunction vitamin deficiency order generic extra super avana on-line see survival through the economic downturn and to erectile dysfunction what to do cheap extra super avana 260mg with amex prepare for the demographic challenges emerging. The aspiration was for the employment rate to reach 70% for men and over 60% for women by 2010, thus moving towards the reduction of the gender inequalities that had existed. Building on this the Europe 2020 strategy for jobs 8 and growth was adopted in June 2010 with the aim of raising to 75% the 8 http://ec. Amongst its other aims it set to improve education levels, in particular by aiming to reduce school drop-out rates to less than 10% and by increasing the share of 30-34 years old having completed tertiary or equivalent education to at least 40%. By 2007 good progress was being made with more women entering the workforce and a period of relative stability saw an increase in men�s jobs. In Estonia, Latvia and Lithuania there is a higher proportion of 69 women in full time employment and in the majority of the Eastern European countries there are more men in part-time work than women. This highlights a feature of the most recent recession across Europe in 71 that it seems to have hit male employment quite hard due to manufacturing being much more affected than services, especially engineering and the construction industries, which employ many more men (Eurostat, 2010b). The current picture shows that Latvia has nearly 11% of its male population in long term unemployment whereas Norway has less than 1% (see Fig. There are some countries where the male employment has gone up, but the majority are seeing a fall. When this is coupled with the fact that we are also seeing a rapid ageing of the workforce the ability for industry to keep their older men in the workforce for longer is of prime importance. The migratory process as well as the economic and social conditions of migrants can have a negative impact on health. Many of health problems of migration relate to the specific features of health care utilisation. The health of migrants might have significant social and economic consequences for host countries as well. Social, economic, cultural and linguistic barriers may pose obstacles using health services and to the capacity of services to meet the needs of migrant workers. Many studies have shown that chronic diseases are less prevalent in some migrant groups compared to host European populations. Many European countries have selection processes which deny admission to individuals with existing illness or support self-selection of healthier individuals. Another reason relates to a difference in timing between the health benefits and the health risks of migration. For several conditions, many migrants may display better health indicators than the host population. However, over time these advantages 74 decrease and migrants begin to assume the characteristics of the host populations. The healthy immigrant effect is in fact on the basis of the literature a consequence of several health and social factors. Many immigrants arrive from regions of the world where lifestyle-associated risk factors contributing to chronic diseases, particularly obesity, inactivity and diet, are less prevalent than those observed in the developed world. European countries that have complex immigration selection processes often search for younger and better educated immigrants, who may also be better able than older, less healthy immigrants to cope successfully with the physical, psychological and sociological challenges of immigration. Immigration medical requirements and screening for chronic diseases may deny admission to individuals with existing illness or support self- selection of healthier individuals. For several conditions and illnesses, many migrants, for example, on arrival, 9 display better health indicators than the host population. Longitudinal studies in some major receiving countries suggest that over time these advantages decrease and migrants begin to assume the characteristics of the host populations. Studies on this effect in Europe are limited but there is growing evidence of the healthy migrant effect in several conditions. The following explanations for the differences in health between ethnic groups have been identified � genetic differences; � cultural differences; � socioeconomic position; � short term migration history; � ethnic identity. On arrival being in hazardous working and living conditions coupled with being unaware of how the host countries health services works and younger men�s attitudes to risk taken and reluctance to seek help makes them particularly vulnerable (Carballo & Mboup, 2005) (see also Section 1. There are nine countries where more women leave: these tend to be in Eastern Europe. In all countries there are higher numbers of male asylum seekers compared to female (Fig. These include: population stocks and general demographic characteristics, migration flows, residence permits, acquisition and loss of citizenship, asylum seekers and refugees, irregular migration, employment, income, transfers and social benefits, housing and residential patterns, health and access to healthcare, education, family and household, political participation and crime and justice. Those entering the criminal justice system have been often been subjected to a lifetime of social exclusion, including poor educational backgrounds, low incomes, meagre employment opportunities, lack of engagement with normal societal structures, low self- esteem and impermanence in terms of accommodation (including bouts of homelessness) and relationships with family members (Social Exclusion Unit, 2002). Examples include long periods of time locked in a cell; overcrowded conditions; a lack of privacy; limited autonomy, choice or control; bullying and violence and limited amounts of exercise (Woodall, 2010a). Paradoxically, prisons can be both places of health risk and health improvement for men. Prisons can offer the opportunity for rehabilitation, both in terms of tackling the high proportion that go on to re-offend. They can also give opportunities for working with men to help to improve their health and well-being. Prisons can represent an escape from the toxic environments from which many prisoners have come, whilst drug rehabilitation and the teaching of life skills such as anger management and work skills can provide a basis for the successful re- integration within society (Woodall, 2010b). Currently, thirty-eight countries across Europe are participating at a policy making level to reduce public health risks through improving health in prisons (Moller at al. There are many reasons for experiencing homelessness and housing deprivation, which include: � structural factors, such as lack of access to, or unavailability of, affordable housing; limited access to the labour market; lack of social services; � social factors, such as barriers to social inclusion or the marginalisation of a particular group in society; � personal factors, such as poor mental health, alcohol or drug addiction, a low level of education and lack of qualifications, gambling problems, a criminal record, exposure to domestic violence or lack of family support. The numbers who are affected are difficult to determine, as many do not enter the official statistics as many countries do not collect the data or use differing definitions of homelessness (Edgar & Meert, 2006). Though many women are affected by homelessness (often as a result of domestic violence). A study in the Netherlands found that 88% of the homeless were men (van Laere et al. There is a particular problem with men who have found it difficult making the transition from an institution back in to civilian life. A high number of ex- servicemen are affected by this through a combination of alcohol abuse and the reaction to the psychological trauma makes it difficult for families to cope and they end up homeless (Busuttil, 2010). Prison leavers are also a group who feature high in the data on the homeless, with 34% of London�s rough sleepers having been in prison. Some of their problems are due to their lack of accommodation prior to imprisonment, some due to losing tenancy whilst in custody and for others due to loss of family contact as a result of their crimes (Social Exclusion Unit, 2002). Immigrants are also at risk (Edgar & Meert, 2006) through their precarious working conditions as outlined above or through arriving in a country without accommodation or support being available. In some countries, illegal immigrants constitute the greatest proportion of those sleeping rough or using overnight shelters, the majority of whom are male. This support is not only crucial in preventing them ending up on the street but also in enabling them to get out of the situation they are in, in particular to find a job and to avoid becoming marginalised in society� (Eurostat, 2010a, p 179) 81 Services are being set up to cater for homeless men (see for example McCullagh, 2010) but these are limited, with many countries having no specific assistance for men or programmes in place to help prevent men who are at risk of homelessness or are on the streets already. Disability comes in many forms and men are seen to have high levels of accident and work related disability. For instance it is estimated that about 7% of European workers have some form of work related hearing problem. With the changes in modern warfare and improvements in battlefield health care there are a significant number of young men returning from conflict with severe disabilities. Improvements in the care of the young disabled have resulted in a growing number of men entering adulthood with profound physical and learning disabilities. In addition to these men with very special physical and emotional health needs there are a much larger cohort of men with mild to moderate learning difficulties trying to negotiate themselves through an increasingly complex society (Cambridge & Mellan, 2000; Elliott at al. Oxford, Radcliffe Publishing Cambridge P, Mellan B (2000) Reconstructing the sexuality of men with learning disabilities: Empirical evidence and theoretical interpretations of need. Disability & Society 15:293-311 Carballo M, Boup M (2005) International migration and health A paper prepared for the Policy Analysis and Research Programme of the Global Commission on International Migration. Polity Press, Cambridge Council Directive (2010) European Commission available at: http://eur- lex.
Trimethoprim- sulfamethoxazole induced hyperkalaemia in elderly patients receiving spironolactone: nested case-control study erectile dysfunction caused by vasectomy buy extra super avana 260mg on-line. Trimethoprim-sulfamethoxazole and risk of sudden death among patients taking spironolactone erectile dysfunction 34 purchase extra super avana now. June 17 erectile dysfunction liver cirrhosis generic 260 mg extra super avana with mastercard, 2016 86 Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People 15 erectile dysfunction miracle shake buy generic extra super avana pills. Providers should screen all transgender people for hepatitis C risk factors and perform an antibody screen in those determined to be at risk, as per current guidelines. All transgender people who inject soft tissue fillers should be screened for hepatitis C. Both estrogen and testosterone undergo hepatic metabolism, and routine monitoring of hepatic function has been recommended. However, neither hormone has been associated with hepatic injury or abnormal liver function tests. Monitoring of liver function in patients with chronic hepatitis C infection should proceed as routinely recommended by disease stage and risk factors for progression dictate. Non-oral forms of hormone therapy avoid first pass through liver metabolism and may be preferred for patients with liver disease, though there is no specific evidence to support this recommendation. However, methyltestosterone is no longer available in most countries and should no longer be used as part of a gender-affirming hormone regimen. Oral testosterone undeconoate gel caps available outside the United States were not associated with hepatic dysfunction in a 10-year safety study among non-transgender males. June 17, 2016 87 Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People Table 15-1. Co-administration of ethinyl estradiol with boceprevir or telaprevir was found to decrease estrogen levels. In summary, ethinyl estradiol is contraindicated with ombitasvir/paritaprevir/ritonavir. June 17, 2016 88 Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People References 1. Drug-drug interaction profile of the all-oral anti-hepatitis C virus regimen of paritaprevir/ritonavir, ombitasvir, and dasabuvir. Screening intervals should be based on risk, with screening every three months in individuals at high risk (multiple partners, condomless sex, transactional sex/sex work, sex while intoxicated). In practice, transgender people may avoid screening procedures and physical examinations due to fear of discrimination,[3] encountering providers who are inadequately trained in transgender health,[4] or personal discomfort with the visit or exam. Because transgender people differ in hormone use, history of gender-affirming surgical procedures, and patterns of sexual behavior, providers should avoid making any assumptions about presence or absence of specific anatomy; sexual orientation; or sexual practices. To facilitate a respectful rapport, use the patient�s preferred terminology to refer to anatomic parts. The Fenway Guide provides suggested sexual risk assessment questions [6] including: � Are you having sex? These questions are components of a complete sexual history which would include relationship types, frequency of sexual activity, age of sexual debut, use of drugs or alcohol during sex, sex work history, history of sexual abuse, and sexual function. Self-collected vaginal and rectal swabs as well as urine specimens have equivalent sensitivity and specificity to provider-collected samples for nucleic acid amplification testing for gonorrhea, chlamydia, and trichomonas. Some surgical approaches include the use of urethral tissue, which could result in mucosal infectious such as chlamydia or gonorrhea. The risk of infection of intact, inverted penile skin with these organisms is unknown, though lesions such as a syphilitic chancre, herpes or chancroid are possible. When clinically indicated due to symptoms, a physical examination and appropriate testing should be performed. The anatomy of a neovagina created in a transgender woman differs from a natal vagina in that it is a blind cuff, lacks a cervix or surrounding fornices, and may have a more posterior orientation. The anoscope can be inserted, the trocar removed, and the vaginal walls visualized collapsing around the end of the anoscope as it is withdrawn. There is no evidence to guide a decision to perform routine pelvic exams on transgender women in order to screen for such conditions as [formerly penile skin] warts or lesions. Transgender women who have undergone vaginoplasty retain prostate tissue, therefore infectious prostatitis should be included in the differential diagnoses for sexually active trans women with suggestive symptoms. There is no evidence to guide routine screening for Chlamydia in asymptomatic transgender women who have undergone vaginoplasty, though it is reasonable to consider urinary screening in women with risk factors. The role of vaginal gonorrhea and Chlamydia specimens, as opposed to urine testing only, is unknown in women June 17, 2016 91 Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People who have undergone penile inversion. Providers may consider vaginal testing however urine testing should be considered essential. Pelvic inflammatory disease should be in the differential for transgender men with a uterus and fallopian tubes who have vaginal intercourse. Testosterone use is associated with vaginal atrophy; therefore, use of lubricant and a small speculum may be appropriate for pelvic and speculum exams among transgender men with vaginas. Some transgender men retain patent vaginas after metoidoplasty and may require vaginal screening based on sexual history. Trauma informed care in medicine: current knowledge and future research directions. June 17, 2016 92 Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People 17. A common cause of scrotal contents pain in transgender women is �tucking,� which allows a female-appearing genital contour in tight fitting clothing. Tucking involves manually displacing the testes upward in to the inguinal canal, and then positioning the penis and scrotal skin between the legs and rearward toward the anus. Tight underwear, tape or a special garment known as a gaff is then used to maintain this positioning. Many transgender women find this practice to be gender-affirming, and may maintain this positioning even at night when asleep. Prolonged tucking may also result in urinary reflux and symptoms of prostatism or even infection such as epididymo- orchitis, prostatitis, or cystitis. Prolonged positioning of a compressed urethral meatus in close approximation to the anus may also serve as a portal of infection. Pain related to the onset of hormone therapy is a common complaint however the etiology of this symptom is unknown. Acute scrotal contents pain requires a workup to rule out conditions requiring emergency treatment. A physical exam to rule out tumors, hernia, hydrocele or other causes of pain is appropriate. Ready access to transgender surgeries when medically necessary, including orchiectomy and vaginoplasty for the treatment of gender dysphoria, may also minimize this condition. Chronic orchialgia algorithms for non-transgender men often suggest an empirical course of antibiotics (after attempting diagnosing an etiology) and discourage orchiectomy as a last resort measure. Patients often have gender dysphoria and maybe relieved to be offered orchiectomy (as opposed to non- transgender men, who are typically resistant to even unilateral orchiectomy when indicated); orchiectomy may be raised much higher in the treatment algorithm in these cases. When orchiectomy is not indicated, medications used in the treatment of neuropathic pain may be June 17, 2016 93 Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People useful. Pain related to onset of hormone therapy is generally benign, improves spontaneously, and can be treated expectantly and with reassurance. Providers should not discount testicular pain complaints in transgender individuals, and should avoid any perception that transgender women with this complaint are malingering in hope of obtaining an orchiectomy. June 17, 2016 94 Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People 18. Army staff noticed that drums of Dow 200 silicone lubricant were disappearing from supply rooms, and traced these drums to providers who were injecting the material. By the 1960s, Dow Chemical had introduced a purified medical silicone (Dow 360), intended for use as a syringe lubricant and as a pharmaceutical vehicle. Subsequent off-label use of Dow 360 was associated with a number of poor outcomes, and by the 1970s some laws had been passed banning the use of such injections. The actual composition of the injected substances is often unknown and may not be of medical grade; contents may include aircraft lubricant, tire sealant, window caulk, mineral oil, methylacrylates, petroleum jelly, or other substances.
Therapeutic strategies for reductase inhibitor dutasteride on localized prostate cancer - drug treatment of stress urinary incontinence. Low evidence of radiation therapy in treatment of erectile dysfunction in patients with prostate cancer: A plea for intensified scientific activity. Abdominal electric stimulation facilitates Archer S L, Gragasin F S, Webster L et al. Aetiology penile vibratory stimulation for ejaculation after spinal cord and management of male erectile dysfunction and injury: a single-subject trial. Archives of Physical Medicine & female sexual dysfunction in patients with Rehabilitation 2005;86(9):1879-1883. Italian Heart Journal: Official Journal of the Italian Federation of Cardiology Atala A, Amin M. The diabetes physician and an assessment and treatment programme for male erectile impotence. Erectile dysfunction: Expectations beyond phosphodiesterase Type 5 Anderson P C B, Gommersall L, Hayne D et al. Expert Opin Drug Saf 2004;3(5):457� for erectile dysfunction: evolving concepts with 470. Changing practice patterns in erectile dysfunction: a diagnostic algorithm for the new Beckman T J, bu-Lebdeh H S, Mynderse L A. Intracavernous pharmacotherapy for Core document on erectile dysfunction: Key aspects in erectile dysfunction. Contemporary intracavernous pharmacotherapy for erectile dysfunction in the aging male. Erectile dysfunction in uremic dialysis patients: Diagnostic evaluation in the Burns-Cox N, Gingell C. Psychosomatic aspects in the diagnosis and treatment Geriatrics 1994;49(10):27-32. Expert Opinion on Endocrinology & Metabolism Clinics of North Emerging Drugs 2004;9(1):179-189. Cardiac safety in clinical trials of European Urology Supplements 2002;1(8):12-18. Erectile dysfunction: Evaluation and new treatment Corbin J D, Francis S H, Webb D J. Transurethral therapy for the treatment of erectile dysfunction: Infant or dinosaur?. Cardiac safety in clinical trials of approach to erectile dysfunction in spinal cord injured phosphodiesterase 5 inhibitors. Erectile dysfunction and cardiovascular disease: potentially useful as peripheral vasodilator agents. Advanced Studies in Journal of Enzyme Inhibition & Medicinal Chemistry Medicine 2006;6(4):163-170. Rosen, Raymond C (Ed); Leiblum, Sandra Risa (Ed) 1992;(1992):378 Chaudhuri A, Wiles P. Do vardenafil and tadalafil have advantages over sildenafil in the treatment of erectile dysfunction?. How, why and when should Peet, Malcolm (Ed); Wilson, Catherine (Ed) urologists evaluate male sexual function?. The etiology of erectile dysfunction and mechanisms by which drugs improve Dunsmuir W D, Holmes S A. Nitric therapy for symptomatic late-onset hypogonadism with oxide pathway and phosphodiesterase inhibitors in transdermal testosterone gel. From 1998;59(10):777 informed consent through database lock: An interactive clinical trial conducted using the internet. Eur Heart J Suppl Levine, Stephen B (Ed); Risen, Candace B (Ed); Althof, Stanley 2002;4(H):H7-H12. Apomorphine: A sublingual dopamine agonist for the prostatic hyperplasia: Now we can begin to tailor treatment of erectile dysfunction. Sexual dysfunction in patients with Prostate Cancer & Prostatic Diseases 2003;6(4):268� hypertension: implications for therapy. Lecture 5: Sexual dysfunction in the Godschalk Michael F, Sison Alfredo, Mulligan Thomas. Patient preferences in treatment of erectile dysfunction: the continuing importance of Gonzalez R R, Kaplan S A. Clinical implications of antidepressant drug effects on sexual Greiner K A, Weigel J W. Current treatments and emerging therapeutic approaches in male erectile dysfunction. Factors in predicting initial in-office therapeutic dosages of alprostadil for the treatment of Heaton J P. Treatment for erectile dysfunction based future: a 7-year update of Viagra (sildenafil citrate). New perspectives in agents for self-injection programs and alternative application the pharmacotherapy of erectile dysfunction. Andropause: is androgen pharmaceutical profiles for clinical studies on erectile replacement therapy indicated for the aging male?. Gonadal tonic contraction in the treatment of erectile and erectile dysfunction in diabetics. Journal fur Urologie und Urogynakologie American Journal of Cardiovascular Drugs 2005;5(1):31-39. Testosterone therapy - What, when Journal of Diabetes & Vascular Disease 2004;4(6):383-386. Update on oral treatments for of sildenafil metabolism may promote nitrate-induced male erectile dysfunction. Sex and the patient with cardiovascular for the treatment of male erectile dysfunction. Novel Phosphodiesterase Type 5 dysfunction and active depression: an analytic cross-sectional Inhibitors: Assessing Hemodynamic Effects and study of general medical patients. Erectile dysfunction and cardiovascular - Statistical significance may not translate into clinical risk factors. Recent advances in the treatment of erectile dysfunction in patients with Kendirci M, Bejma J, Hellstrom W J G. Epidemiology prostaglandins in the aetiology and treatment of erectile of erectile dysfunction. Tadalafil: An oral selective and its inhibitors: Update on pharmacological and phosphodiesterase 5 inhibitor for treatment of erectile therapeutical aspects. Noninvasive management of lower urinary tract symptoms and sexual dysfunction Kirby M. Management of erectile dysfunction in men with associated with benign prostatic hyperplasia in the cardiovascular conditions. Curr Opin Urol 2003;13(5):405� with benign prostatic hyperplasia and erectile dysfunction. Pharmacotherapy for erectile erectile dysfunction: what to look for and when to treat. Management of sexual dysfunction in erectile disorders: Conceptual and clinical considerations. Non-surgical management of Sexuality, Reproduction & Menopause 2003;1(1):40� erectile dysfunction. Review of intraurethral suppositories and erectile dysfunction following radical prostatectomy. Nutrients and botanicals for erectile dysfunction following spinal cord injury: a review. Expert Review of Neurotherapeutics Myocardial infarction following the combined 2003;3(5):641-648. Management of erectile dysfunction by the primary correlate positively with measures of emotional well� care physician. Geriatrics and Aging 2004;7(6):23� the patient with prostate cancer about treatment- 28.
Generic 260mg extra super avana with visa. Erectile Function Exam ASMR.