

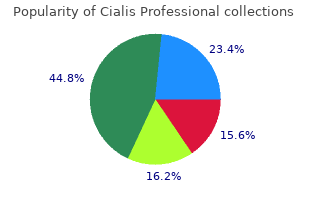
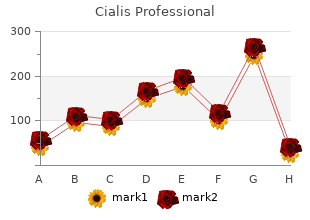
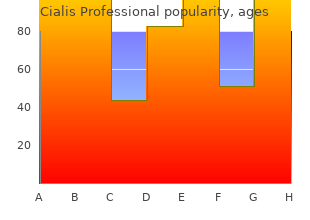
Cialis Professional
"Buy cialis professional on line amex, erectile dysfunction and diabetes leaflet."
By: Denise H. Rhoney, PharmD, FCCP, FCCM
- Ron and Nancy McFarlane Distinguished Professor and Chair, Division of Practice Advancement and Clinical Education, UNC Eshelman School of Pharmacy, Chapel Hill, North Carolina

https://pharmacy.unc.edu/news/directory/drhoney/
Main side effects: � fatulence and abdominal bloating � nonresponse to impotence and prostate cancer buy cialis professional australia carbohydrates other than glucose if hypoglycaemic � (rare) liver abnormalities impotence yoga buy generic cialis professional 20mg. Glitazones (pioglitazone and rosiglitazone) Prospective cardiovascular trial data exists erectile dysfunction treatment after prostatectomy 40 mg cialis professional free shipping. Glitazones: � sensitise the liver and peripheral tissues to impotence yoga order 40 mg cialis professional mastercard insulin and are effective in lowering blood glucose by reducing insulin resistance � can (both pioglitazone and rosiglitazone) be used as combination therapy with metformin or sulphonylureas or insulin. Contraindications (for both pioglitazone and rosiglitazone): � moderate to severe cardiac failure � increased risk of bladder cancer. General practice management of type 2 diabetes 145 Main side effects: � nasopharyngitis � headache � upper respiratory tract symptoms. Main side effects: � weight loss � increased urogenital and urinary tract infections � aggravate dehydration. An empirical approach to dosage together with a �go slow� policy will result in the smoothest fine-tuning of management. Some of these insulins are available as injection devices, pen injectors, disposable insulin pens, cartridges and vials. General practice management of type 2 diabetes 147 Appendix I: Examples for insulin initiation and titration 87,185 I. Halve the current once daily insulin dose and give the reduced dose twice daily; pre-breakfast and pre-dinner 2. If HbA1c is not at target after 3 months add a further prandial insulin dose to another meal (e. Add a new rapid-acting (prandial) insulin to the next largest meal of the day (starting at 10% of the basal insulin dose or 4 units) 3. Hypoglycaemia can lead to falls, fractures, injuries, arrhythmias and, in severe cases, death. Hypoglycaemia occurs most frequently with: � insulin therapy � sulphonylurea therapy � defcient carbohydrate intake � unaccustomed exercise. The risk of hypoglycaemia with each sulphonylurea relates to its pharmacokinetic properties. Studies have shown signifcantly lower rates of hypoglycaemia associated with the use of gliclazide (Diamicron) compared with other sulphonylureas. General practice management of type 2 diabetes 151 Although many newer therapies for type 2 diabetes do not cause hypoglycaemia when used as monotherapy, their use in combination with insulin or sulphonylureas increases the risk of hypoglycaemia. The use of insulin analogs may limit, but not eradicate, the risk of hypoglycaemia. Common symptoms fall in to two categories: adrenergic symptoms of trembling or shaking, sweating, hunger, lightheadedness and numbness around the lips and fngers, and neuro-glycopaenic symptoms of lack of concentration, weakness, behavioural change, tearfulness/crying, irritability, headache and dizziness. Severe hypoglycaemia occurs clinically when a patient requires external assistance from another person to manage an episode of hypoglycaemia. Hypoglycaemic unawareness is of particular concern and refers to the clinical situation where a patient loses the ability to detect the early symptoms of hypoglycaemia. This results from repeated episodes of mild hypoglycaemia with eventual loss of adrenergic and neuro-glycopaenic symptoms. It can lead to confusion and marked behavioural change which is not recognised by the patient and may progress to loss of consciousness. The cause needs to be identifed and the episode dealt with by reinforcing education, counselling the patient and perhaps changing treatment. Management of an episode of hypoglycaemia If a patient with diabetes is showing signs of potential hypoglycaemia, frst make sure the patient is safe (e. If the level is not rising, suggest eating another quick-acting carbohydrate from the above list. If the patient is symptomatic but the blood glucose or capillary glucose cannot be performed to confrm the episode is due to hypoglycaemia, treat the patient as if they have hypoglycaemia by administering 15 g of quick-acting carbohydrate. If there is no improvement after 15 minutes, the patient could have another cause for the episode and further medical assistance may be necessary. If the patient cannot safely swallow 15 g of carbohydrate due to their depressed mental state, consider the administration of 1 vial of glucagon intramuscularly, if available. If glucagon is administered, always review the monitored capillary glucose after 15 minutes to ensure effective management of the hypoglycaemia has occurred and the blood glucose remains above 4 mmol/L. Post-hypoglycaemia: Re-assess the patient�s circumstances, medication dosages, and dietary intake as well as overall need for glucose monitoring after any severe hypoglycaemic episode with both the patient and/or with their immediate family or support persons. Also ensure implications for driving competence, operation of machinery and other similar areas are discussed with the patient. Hyperglycaemic emergencies should be preventable in people known to have diabetes, and their occurrence in this group signifes a major breakdown in medical management. Adequate early management of sick patients with diabetes will prevent the development of hyperglycaemic emergencies. This results in: � increasing hepatic glucose production causing hyperglycaemia � increasing peripheral lipolysis releasing free fatty acids. These are converted to ketoacids by the liver resulting in a metabolic acidosis � hyperglycaemia-induced osmotic diuresis leading to sodium, potassium and phosphate depletion � dehydration causing pre-renal failure. Urinalysis can be used for initial assessment if blood ketone testing is not available. Additionally associated problems arising from or precipitating the episode need to be addressed. In this situation it is advisable to contact the most appropriate diabetes resource person for advice while commencing treatment promptly. Fluid replacement with normal saline and potassium should continue for at least the frst 6 hours. Run 100 mL through the line before connecting to the patient to saturate insulin binding to the giving set. If a syringe pump is available add 50 units of neutral insulin to 50 mL of saline and fush the giving set. Once treatment is initiated (unless the acidosis is mild and response rapid) transfer the patient to a specialist unit. This is usually a result of illness or infection, however it can also be due to poor patient compliance. Signifcant insulin defciency causes hyperglycaemia due to increased hepatic gluconeogenesis. However, as absolute insulin defciency is not present, peripheral lipolysis remains suppressed and the release of free fatty acids is low. Little substrate is available for generation of ketoacids and a metabolic acidosis does not occur. Eventually, severe intravascular volume depletion occurs resulting in a further deterioration of renal function. Consequently glomerular fltration diminishes preventing the further excretion of glucose. With ongoing increased hepatic glucose production, decreased peripheral glucose utilisation and reduced urinary glucose losses, severe hyperglycaemia results. The priority is to correct the extracellular fuid defcit, then slowly correct the hyperglycaemia (with insulin) and water defcit (with low sodium fuids [e. It is important to note that blood glucose meters do not register very high glucose levels so access to a laboratory is necessary to monitor the correction of hyperglycaemia as well as to monitor sodium and potassium levels. Patients who are unable to eat should continue to receive intravenous insulin infusion and fuid replacement. Some patients with type 2 diabetes may 1- 195 be treated with oral anti-diabetic agents and lifestyle modifcation after recovery. In patients with potential complications of hypophosphatemia the use of phosphate maybe justifed. Potassium replacement may be given 2++ 189 1/3 as potassium phosphate and 2/3 as potassium chloride. Serum calcium level should be monitored in 2++ 199 patients receiving phosphate infusion. Education of the diabetic patient and care 1� 201, 202 givers on the process of care and sick day management. Partnering with patients and families to design a patient- and family-centered healthcare system: recommendations and promising practices. Safety and quality improvement guide Standard 1: Governance for Safety and Quality in Health Service Organisations (October 2012). Outcomes of implementing patient centred medical home interventions: a review of the evidence from prospective studies in the United States.
Study discontinuation occurred more frequently in patients who received add-on combination ther- apy than in those who received placebo add-on (4 erectile dysfunction doctors long island purchase cialis professional 40mg overnight delivery. Other studies found no difference in discontinuation rates due to erectile dysfunction massage discount 20mg cialis professional mastercard drug-related adverse events (Table 55) (163 erectile dysfunction pills for sale generic 40mg cialis professional overnight delivery,164) erectile dysfunction treatment adelaide cheap cialis professional online mastercard. Antimuscarinic adverse events such as dry mouth and constipation occurred in the combi- nation therapy group more often than with alpha1-blocker monotherapy (162,163,165,353,358). However, in most studies, side effects were mild and improved on drug discontinuation (162,353). Astellas Pharma has sponsored a 12-week randomized trial using different dosages of solifenacin with 0. Male Lower Urinary Tract Symptoms: Medical Management and New Therapeutic Targets 513 8. These studies do not feature a placebo control arm, are of short duration, and have a limited number of patients enrolled. Sexual Health Inventory for Men scores had a significantly greater improvement in both the sildenafil-only (65%) and the combination (67. This study showed that treatment with the combi- nation of tamsulosin and sildenafil was not superior to monotherapy with tamsulosin (365). There were no differences in the incidence of common, treatment-related adverse events between men undergoing combined therapy and those receiving tamsulosin alone (366). Additional higher-quality controlled studies are needed before recommen- dations can be made (Grade D). United Nations, Department of Economic and Social Affairs, Population Division (2011). The standardisation of terminology in lower urinary tract function: Report from the standardisation sub-committee of the International Continence Society. Correlation of the American Urological Association symptom index with self-administered versions of the Madsen-Iversen, Boyarsky and Maine Medical Assessment Program symptom indexes. The American Urological Association symptom index for benign prostatic hyperplasia. Epidemiology and natural history of benign prostatic hyperplasia: 4th International Consultation on Benign Prostatic Hyperplasia. Etiology, pathophysiology, epidemiology and natural history of benign prostatic hyperplasia. Male Lower Urinary Tract Symptoms: Medical Management and New Therapeutic Targets 517 22. Analytical accuracy and reliability of commonly used nutritional supplements in prostate disease. Not all brands are created equal: A comparison of selected components of different brands of Serenoa repens extract. Inhibition of androgen metabolism and binding by a liposterolic extract of �Serenoa repens B� in human foreskin fibroblasts. Effects of the lipidosterolic extract of Serenoa repens (Permixon) on human prostatic cell lines. The lipidosterolic extract from Serenoa repens interferes with prolactin receptor signal transduction. Anti-edematous action of a hexane extract of the stone fruit of Serenoa repens Bartr. Updated meta-analysis of clinical trials of Serenoa repens extract in the treatment of symptomatic benign prostatic hyperplasia. Meta-analysis of clinical trials of Permixon in the treatment of symptomatic benign prostatic hyperplasia. Saw palmet to extracts for treatment of benign prostatic hyperplasia: A systematic review. Activity and isolated phytoestrogen of shrub palmet to fruits (Serenoa repens Small), a new estrogenic plant. A double-blind trial of an extract of the plant Serenoa repens in benign prostatic hyperplasia. A double-blind, placebo-controlled study of the plant extract Serenoa repens in the treatment of benign hyperplasia of the prostate. Saw palmet to (Serenoa repens) in men with lower urinary tract symptoms: Effects on urodynamic parameters and voiding symptoms. Efficacy and tolerability of the lipidosterolic extract of Serenoa repens (Permixon) in benign prostatic hyperplasia: A double-blind comparison of two dosage regimens. Early urodynamic effects of the lipido-sterolic extract of Serenoa repens (Permixon(R)) in patients with lower urinary tract symptoms due to benign prostatic hyperplasia. A randomized, double-blind, placebo-controlled trial to determine the effectiveness of botanically derived inhibitors of 5-alpha-reductase in the treatment of androgenetic alopecia. Serenoa repens extract for benign prostate hyperplasia: A randomized controlled trial. Effect of increasing doses of saw palmet to extract on lower urinary tract symptoms: A randomized trial. Comparison of phytotherapy (Permixon) with finasteride in the treatment of benign prostate hyperplasia: A randomized international study of 1,098 patients. Comparison of a phytotherapeutic agent (Permixon) with an alpha-blocker (Tamsulosin) in the treatment of benign prostatic hyperplasia: A 1-year randomized international study. Comparison of finasteride (Proscar), a 5a reductase inhibitor, and various commercial plant extracts in in vitro and in vivo 5a reductase inhibition. Antiproliferative effect of Pygeum africanum extract on rat prostatic fibroblasts. Effect of Pygeum africanum extract on A23187-stimulated production of lipoxygenase metabolites from human polymorphonuclear cells. A Pygeum africanum extract with so-called phyto-estrogenic action markedly reduces the volume of true and large prostatic hypertrophy. Effects of Tripterygium wilfordii hook F extracts on induction of cyclooxygenase 2 activity and prostaglandin E2 production. Protective effect of Tadenan on bladder function secondary to partial outlet obstruction. Efficacy of Pygeum africanum extract in the medical therapy of urination disorders due to benign prostatic hyperplasia: Evaluation of objective and subjective parameters. Controlled study of the effects of Pygeum africanum extract on the functional symptoms of prostatic adenoma. Comparison of once and twice daily dosage forms of Pygeum africanum extract in patients with benign prostatic hyperplasia: A randomized, double-blind study, with long-term open label extension. Medical treatment of fibroadenomatous hypertrophy of the prostate with a new plant substance. Male Lower Urinary Tract Symptoms: Medical Management and New Therapeutic Targets 519 65. Treatment of outflow tract obstruction due to benign prostatic hyperplasia with the pollen extract, cernilton. In vitro evaluation of the pollen extract, Cernitin T-60, in the regulation of prostate cell growth. Results of treatment with pollen extract (Cernilton N) in chronic prostatitis and prostatodynia. A systematic review of Cernilton for the treatment of benign prostatic hyperplasia. Effect of ?-sitosterol (Harzol�) on the expression and secretion of growth factors in primary human prostate stromal cell cultures in vitro. Effect of beta-sitosterol on transforming growth factor-beta-1 expression and translocation protein kinase C alpha in human prostate stromal cells in vitro. Ergebnisse einer Doppelblindstudie ueber die Wirksamkeit von Docosanol und beta-Sitosterin zur konservativen Benhandlung des Prostataadenoms. Therapeutische Erfahrungen mit beta-Sitosterin (Prostasal) zur konservativen Behandlung des Prostataadenoms. Ergebnisse einer randomisierten Doppelblindstudie uber die Behandlung der benignen Prostatahyperplasie mit Prostagutt versus beta-Sitosterin. Randomised, placebo-controlled, double-blind clinical trial of beta-sitosterol in patients with benign prostatic hyperplasia.
For several conditions, many migrants may display better health indicators than the host population. However, over time these advantages 74 decrease and migrants begin to assume the characteristics of the host populations. The healthy immigrant effect is in fact on the basis of the literature a consequence of several health and social factors. Many immigrants arrive from regions of the world where lifestyle-associated risk factors contributing to chronic diseases, particularly obesity, inactivity and diet, are less prevalent than those observed in the developed world. European countries that have complex immigration selection processes often search for younger and better educated immigrants, who may also be better able than older, less healthy immigrants to cope successfully with the physical, psychological and sociological challenges of immigration. Immigration medical requirements and screening for chronic diseases may deny admission to individuals with existing illness or support self- selection of healthier individuals. For several conditions and illnesses, many migrants, for example, on arrival, 9 display better health indicators than the host population. Longitudinal studies in some major receiving countries suggest that over time these advantages decrease and migrants begin to assume the characteristics of the host populations. Studies on this effect in Europe are limited but there is growing evidence of the healthy migrant effect in several conditions. The following explanations for the differences in health between ethnic groups have been identified � genetic differences; � cultural differences; � socioeconomic position; � short term migration history; � ethnic identity. On arrival being in hazardous working and living conditions coupled with being unaware of how the host countries health services works and younger men�s attitudes to risk taken and reluctance to seek help makes them particularly vulnerable (Carballo & Mboup, 2005) (see also Section 1. There are nine countries where more women leave: these tend to be in Eastern Europe. In all countries there are higher numbers of male asylum seekers compared to female (Fig. These include: population stocks and general demographic characteristics, migration flows, residence permits, acquisition and loss of citizenship, asylum seekers and refugees, irregular migration, employment, income, transfers and social benefits, housing and residential patterns, health and access to healthcare, education, family and household, political participation and crime and justice. Those entering the criminal justice system have been often been subjected to a lifetime of social exclusion, including poor educational backgrounds, low incomes, meagre employment opportunities, lack of engagement with normal societal structures, low self- esteem and impermanence in terms of accommodation (including bouts of homelessness) and relationships with family members (Social Exclusion Unit, 2002). Examples include long periods of time locked in a cell; overcrowded conditions; a lack of privacy; limited autonomy, choice or control; bullying and violence and limited amounts of exercise (Woodall, 2010a). Paradoxically, prisons can be both places of health risk and health improvement for men. Prisons can offer the opportunity for rehabilitation, both in terms of tackling the high proportion that go on to re-offend. They can also give opportunities for working with men to help to improve their health and well-being. Prisons can represent an escape from the toxic environments from which many prisoners have come, whilst drug rehabilitation and the teaching of life skills such as anger management and work skills can provide a basis for the successful re- integration within society (Woodall, 2010b). Currently, thirty-eight countries across Europe are participating at a policy making level to reduce public health risks through improving health in prisons (Moller at al. There are many reasons for experiencing homelessness and housing deprivation, which include: � structural factors, such as lack of access to, or unavailability of, affordable housing; limited access to the labour market; lack of social services; � social factors, such as barriers to social inclusion or the marginalisation of a particular group in society; � personal factors, such as poor mental health, alcohol or drug addiction, a low level of education and lack of qualifications, gambling problems, a criminal record, exposure to domestic violence or lack of family support. The numbers who are affected are difficult to determine, as many do not enter the official statistics as many countries do not collect the data or use differing definitions of homelessness (Edgar & Meert, 2006). Though many women are affected by homelessness (often as a result of domestic violence). A study in the Netherlands found that 88% of the homeless were men (van Laere et al. There is a particular problem with men who have found it difficult making the transition from an institution back into civilian life. A high number of ex- servicemen are affected by this through a combination of alcohol abuse and the reaction to the psychological trauma makes it difficult for families to cope and they end up homeless (Busuttil, 2010). Prison leavers are also a group who feature high in the data on the homeless, with 34% of London�s rough sleepers having been in prison. Some of their problems are due to their lack of accommodation prior to imprisonment, some due to losing tenancy whilst in custody and for others due to loss of family contact as a result of their crimes (Social Exclusion Unit, 2002). Immigrants are also at risk (Edgar & Meert, 2006) through their precarious working conditions as outlined above or through arriving in a country without accommodation or support being available. In some countries, illegal immigrants constitute the greatest proportion of those sleeping rough or using overnight shelters, the majority of whom are male. This support is not only crucial in preventing them ending up on the street but also in enabling them to get out of the situation they are in, in particular to find a job and to avoid becoming marginalised in society� (Eurostat, 2010a, p 179) 81 Services are being set up to cater for homeless men (see for example McCullagh, 2010) but these are limited, with many countries having no specific assistance for men or programmes in place to help prevent men who are at risk of homelessness or are on the streets already. Disability comes in many forms and men are seen to have high levels of accident and work related disability. For instance it is estimated that about 7% of European workers have some form of work related hearing problem. With the changes in modern warfare and improvements in battlefield health care there are a significant number of young men returning from conflict with severe disabilities. Improvements in the care of the young disabled have resulted in a growing number of men entering adulthood with profound physical and learning disabilities. In addition to these men with very special physical and emotional health needs there are a much larger cohort of men with mild to moderate learning difficulties trying to negotiate themselves through an increasingly complex society (Cambridge & Mellan, 2000; Elliott at al. Oxford, Radcliffe Publishing Cambridge P, Mellan B (2000) Reconstructing the sexuality of men with learning disabilities: Empirical evidence and theoretical interpretations of need. Disability & Society 15:293-311 Carballo M, Boup M (2005) International migration and health A paper prepared for the Policy Analysis and Research Programme of the Global Commission on International Migration. Polity Press, Cambridge Council Directive (2010) European Commission available at: http://eur- lex. European Agency for Safety and Health at Work, Luxembourg, Office for Official Publications of the European Communities Edgar B, Meert H (2006) Fifth review of statistics on homelessness in Europe European Federation of National Organisations working with the homeless. Luxembourg: Publications Office of the European Union 83 Eurostat (2009b) Reconciliation between work, private and family life in the European Union. Luxembourg: Publications Office of the European Union Eurostat (2010a) the Social Situation in the European Union 2009. Luxembourg: Publications Office of the European Union Eurostat (2010b) Combating poverty and social exclusion. Luxembourg: Publications Office of the European Union Flash Eurobarometer (2007) Young Europeans: survey among young people aged 15-30 in the European Union. Frosh S, Phoenix A, Pattman R (2002) Young masculinities: understanding boys in contemporary society. Basingstoke, Palgrave Gatherer A, Moller L, Hayton P (2005) the World Health Organization European health in prisons project after 10 years: persistent barriers and achievements. Houndmills Basingstoke, Palgrave Macmillan Johnson S, Jones A, Rugg J (2008) the Experiences of Homeless Ex-Service Personnel in London Centre for Housing Policy. Global Programme on Evidence for Health Policy Discussion Paper Number 50 McCullough A (2010) Young runaways and adulthood: a difficult transition. J Organiz Behav 31:45�64 Randall G, Brown S (1994) Falling Out: A Research Study of Homeless Ex- Service People. London, Crisis Seiffge-Krenke I (2010) Predicting the timing of leaving the marital home and related developmental tasks: parents� and children�s perspectives. London, Social Exclusion Unit Social Exclusion Unit (2002) Reducing re-offending by ex-prisoners. Men and Masculinities 4(3):258-285 Stephens J (2002) the mental health needs of homeless young people. London, the Mental Health Foundation Walmsley R (2009) World prison population list (8th edn). London, International Centre for Prison Studies Wilson B, Stuchbury R (2010) Do partnerships last? Oxford, Radcliffe Publishing Woodall J (2010b) Control and choice in three category-C English prisons: implications for the concept and practice of the health promoting prison. Higher than advised salt and other mineral levels adds to the negative health consequences of men�s diets. From childhood onwards the lifestyles that many men develop are building up problems for their future, whether it�s smoking, excess alcohol intake, illicit drug use, poor diet or limited physical activity the effect is seen in their high rates of premature death and chronic morbidity. Young men feel they are living invulnerable lives, able to eat, drink and take risks without fear of the consequences; sometimes the reality is immediate, through the sudden death of alcoholic poisoning, or it may be cumulative effect as in the rising incidence of ischemic health disease or cancer in their early adult years. The risks men face are not only the consequence of the life choices they take, there are anatomical and physiological, social and environmental, and service provision factors that can compound the problems. An instance of this relates to the health problems men have when they are overweight, which are a complex blend of the availability of the right food, a socialisation process of boys with regard to their body size and their diet, an increasing sedentary lifestyle coupled with the male form of obesity comprising central (or visceral) fat deposition increasing the risk of the metabolic syndrome and the fat related cancers. This is then linked to the tendency for weight-loss health promotion and services being focused onto women.
Syndromes
- Some warts may cause pain.
- Persons who are severely allergic to the antibiotics neomycin, streptomycin, or polymyxin B. The vaccine contains tiny amounts of these antibiotics.
- CO2
- Oily, foul-smelling, or bloody stools
- Galactosemia
- You are unable to eat or drink for more than 6 - 8 hours
- Spasms of the stomach or intestinal tract
- Blockages in the coronary arteries (coronary artery disease)
- Difficulty breathing
- Epilepsy that involves a part of the brain called the temporal lobe (odor hallucinations are most common)
Three trials utilized fixed doses of alprostadil from 125 to erectile dysfunction age graph generic cialis professional 40 mg without prescription 1000�g administered at 300 erectile dysfunction statistics age purchase 20 mg cialis professional,302 xylometazoline erectile dysfunction discount generic cialis professional uk,304 home based on each subject�s response to erectile dysfunction treatment in thane cheap cialis professional express various doses or a dose titration. The home 302,304 treatment phases of these trials were 3 weeks and 3 months, respectively. In another trial, subjects received single in-clinic administrations of two of four alprostadil doses (125, 250, 500 303 and 1000�g) over a 2 to 4 week period. In a sixth trial, subjects started at either 250 or 500�g alprostadil for 4 weeks with subsequent dose titration so that final dose at 12 weeks ranged from 299 299,300 125 to 1000�g. In one trial that evaluated a prazosin intervention, subjects received single in-clinic administrations of two of four prazosin doses (250, 500, 1000 and 2000�g) over 2 - 4 week 303 period. Study Quality and Reporting 299,300,302� Information on pharmaceutical funding was reported to have been provided for five 304 301 of the six trials. Participant withdrawals, drop-outs or lost to followup were reported in all trials and ranged from 7 percent to 42 percent. The majority of the trials were considered to be of low quality as assessed by the Jadad scale. More commonly reported were quality of erections achieved at home, without regard to whether the patient was able to achieve successful sexual intercourse (�improvement� in erections, �full response,� full erection,� or �grade 4 or 5 erections�). All six trials reported data on penile or urogenital pain and three trials reported results on prolonged erections or priapism/fibrosis. Qualitative Synthesis Summary of qualitative synthesis for this section in presented also in Tables 17-19. In the first trial, compared with men in placebo group, alprostadil-treated men had an increased frequency of penile pain (3. Urinary tract infection occurred in fewer than 1 percent of participants in both groups. No cases of prolonged erection, priapism or fibrosis were observed in either treatment group. There were no cases of priapism or fibrosis, or urinary tract infection in either treatment group. During this period, there was no difference between treatment groups for urethral pain (250�g: 1. Seventy-seven percent of men allocated to an initial dose of 250�g versus 69 percent of those allocated to an initial dose of 500�g elected to increase their dose at 4 weeks. Pooled clinical efficacy results were presented for treatment groups, namely the proportion of men during the study period with at least one successful sexual intercourse attempt (68. In the second trial, there was no statistically significant difference between the two treatment groups with regard to penile pain (25. In this trial, each of 234 participants received single administrations of two of four potential alprostadil doses (125, 250, 500 and 1000�g) and two of four potential prazosin doses (250, 500, 1000 and 2000�g). Results were not provided for the 250�g and 1000 �g alprostadil doses or for the 250�g, 500�g, and 1000�g prazosin doses. Results were not provided for the 250, 500, and 1000�g prazosin doses, though it was stated that 2000�g was the most efficacious prazosin dose. The proportions of patients with penile pain among those allocated to various alprostadil/prazosin combinations were: 23. The corresponding proportions of patients with urethral pain with respect to various alprostadil/prazosin combinations were: 6. Results were not provided for the other six alprostadil/prazosin combinations tested, for the 250 and 1000�g alprostadil doses, or for the 250, 500, and 1000�g prazosin doses. However, it was stated that 500/2000�g was the most efficacious alprostadil/prazosin dose, 500�g was most efficacious alprostadil dose, and 2000�g was the most efficacious prazosin dose. Additional studies of topical testosterone are described in the Hormonal Treatment section. Overview of Trials Of the 12 trials, five reported only physiologic efficacy outcomes, such as in-clinic 307-311 assessment of degree or duration of penile rigidity. The remainder of this section emphasizes results from the seven trials that assessed validated and clinically relevant efficacy 144,306,312-315 outcomes such as sexual intercourse success or improvement in erections at home. Only two trials reported smoking status and none of the trials reported data on obesity. Interventions Topical treatments evaluated in the seven trials that reported clinical efficacy outcomes were 306 313,315 alprostadil, nitroglycerine; aminophylline plus isosorbide dinitrate plus co� 312,314 313 144 dergocrine; minoxidil; and sildenafil. In another, subjects applied a plaster to the penile shaft one hour prior to anticipated sexual activity that released 10 mg nitroglycerine per 24 315 hours. In one trial, subjects applied 1 mL of 2 percent minoxidil solution twice daily on the glans 313 penis. Participants were followed for up to 2 weeks, 144 though it was not clear whether or not they received more than one dose. Study Quality and Reporting Sources of pharmaceutical funding was provided for four trials. Of the trials reporting the clinical efficacy outcomes, only four reported results for sexual intercourse success. Qualitative Synthesis Summary of the results presented in this section is also available in Tables 20�22 Topical Alprostadil versus Placebo. The incidence of adverse events and withdrawals due to adverse events in both patient populations conformed a dose-response trend and that urogenital pain and hypotension occurred numerically more frequently with alprostadil than with placebo. The success rate of vaginal penetration was assessed in two trials of mild to 306 moderate (study a) and severe patients (study b). In the first trial, men allocated to nitroglycerine ointment compared with placebo reported more adverse events (frequent burning at the application site: 12. In the second trial, men allocated to nitroglycerine plaster had more frequent headache (35. In addition, 6 percent of men allocated to nitroglycerine withdrew from therapy due to adverse events (severe pain) versus 0 percent of placebo subjects. One trial (n=132 participants) compared the 313 efficacy and harms of nitroglycerine ointment to minoxidil. Men assigned to received nitroglycerine ointment group reported more frequent side effects than did men in the minoxidil group, including more frequent burning at the application 313 site (12. Topical Aminophylline plus Isosorbide dinitrate plus Co-dergocrine versus Placebo. Two crossover trials compared the efficacy and harms of Aminophylline plus Isosorbide dinitrate 312,314 plus Co-dergocrine versus placebo. None of the patients had prolonged erection or priapism, clinically significant cardiovascular adverse events (such as postural dizziness), headache, or pain at site of 314 312 application. In the second trial, men assigned to the active treatment reported that they experienced erections adequate for intercourse after 3. All successful applications for both the active treatment and placebo 312 groups occurred in a single participant. One crossover trial (n=132) compared the efficacy and harms of 313 minoxidil to placebo. Compared with placebo, men allocated to minoxidil reported more frequent burning at the application site (6 versus 0 percent). No hypotension was reported by either the minoxidil or placebo-treated participants. One trial (n=80) compared the efficacy and 144 harms of topical sildenafil to oral sildenafil. In men assigned to receive topical sildenafil, four (10 percent) reported mild headache. In those assigned to receive oral sildenafil, two participants (5 percent) developed severe headache, one participant (3 percent) reported disturbed visual function, and one participant (3 percent) experienced severe dyspepsia. Quantitative Synthesis No meta-analysis could be performed because of substantial degree of clinical heterogeneity across the trials with regard to patient characteristics, interventions, and the assessed outcomes. Overview of Trials 322,323,326 Three trials used crossover, and the remaining 17 used parallel design. Treatment 319,321,323,330 316 duration in several trials was 6 months and in one trial 12 months. Racial characteristics were reported in only three trials with the majority of the subjects being Caucasians. While trials generally enrolled men with hypogonadism and/or andropause, the specific sexual dysfunction and testosterone entrance criteria across trials varied widely.
Generic cialis professional 20mg mastercard. Show and tell - How to use vacuum erection devices (VEDs) - Lou Rioux.