

Atorvastatin
"Purchase 40mg atorvastatin free shipping, cholesterol blood test fast."
By: Randolph E. Regal, BS, PharmD
- Clinical Associate Professor, Department of Clinical Pharmacy, College of Pharmacy, University of Michigan
- Clinical Pharmacist, University of Michigan Health System, Ann Arbor, Michigan

https://pharmacy.umich.edu/people/reregal
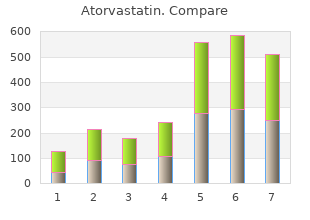
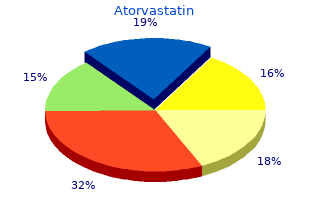
However cholesterol levels recommended uk cheap atorvastatin 5 mg otc, our data showed no difference between the concurrent and sequential types of schizoaffective disorders � on any possible level cholesterol and foods to eat purchase 40 mg atorvastatin free shipping. It may be true cholesterol test variance purchase generic atorvastatin line, then high cholesterol foods grapefruit cheap generic atorvastatin canada, that human beings as well as mental disorders are not a "one-day butterfly" or a "one-night butterfly" but a continuity. Perhaps we cannot explain everything with the facile answer of comorbidity, but perhaps some questions can be answered, at least partially, with refer ence to continuity and longitudinality. It seems certain that schizoaffective disorders are not identical with schizophrenic disorders, although in some individual cases the schizodomi nance is clear. It can also be said that there are some significant differences between schizoaffective and affective disorders in spite of strong similarities (contributions in Marneros and Tsuang 1990 and Marneros 1999). It also seems certain that unipolar affective disorders differ significantly from bipolar affective ones, especially with regard to some relevant socio Bipolar schizoaffective disorders 119 120 A. Rohde demographic and premorbid data and some patterns of course (Angst 1978, 1980a, b, 1986a,b, Angst et al. Differences very similar to those between affective unipolar and affective bipolar patients were found between bipolar and unipolar schizoaffective patients Bipolar schizoaffective disorders 121 122 A. It seems that even after creating two voluminous groups of unipolar and bipolar diseases, each including both affective and schizoaffective disorders, the main differences and similarities between unipolar and bipolar types remain unchanged (Marneros et al. This finding gives further support to the assumption of the two distinct entities, namely unipolar and bipolar diseases, which, however, are phenomenologi cally and prognostically inhomogeneous. Future research must isolate more precisely the reasons for the inhomo geneity of schizoaffective disorders, and discover whether the proportion of schizodominant cases in a sample could be responsible for the differences found between unipolar affective and unipolar schizoaffective disorders, on the one hand, and between bipolar affective and bipolar schizoaffective disorders, on the other. Perhaps, after excluding a schizodominant group, affective and schizoaffective disorders could be classified as two subtypes of a "unipolar disorder" or a "bipolar disorder". It remains to be investi gated whether a schizodominant type of schizoaffective disorders represents a bridge between schizophrenia and bipolar and unipolar diseases (Angst 1986c, Kendell 1986, Marneros 1995). As long as inhomogeneity exists, and the reasons for it are unclear, it is difficult to define a voluminous diagnostic category. Verlauf unipolar depressiver, bipolar manisch-depressiver und schizoaffek tiver Erkrankungen und Psychosen. Bipolar schizoaffective disorders 123 Coryell W, Winokur G Depression spectrum disorders: clinical diagnosis and bio logical implications. Long-term outcome of affective, schizoaffective, and schizophrenic disorders: a comparison. Unipolar and bipolar depression: recent findings from clinical and bio logical studies. Die Gruppirung der psychischen Krankheiten und die Eintheilung der Seelens to rungen. The relationship of schizoaffective illness to schizophrenic and affective disorders. Die Relevanz der Verlaufsdynamik der schizoaffektiven Psychosen fur ihre Prophylaxe und Therapie. Behinderung und Residuum bei schizoaffektiven Psychosen-Daten, methodische Probleme und Hinweise fur zukunftige Forschung. Sociodemographic and premorbid features of schizophrenic, schizoaffective and affective psychoses. The schizoaffective continuum: non-psychotic, mood congruent, and mood incongruent. Pregnancy, the post-partum period and menopause are associated with hormonal changes which occur fre quently in women and seem to trigger the danger of psychic instability in different ways. However, a "protec tive" effect of hormonal changes associated with pregnancy has been dis cussed (Oates 1986). When bipolar disorders do occur in pregnancy, they usually constitute a relapse of a preexisting bipolar disorder, often following a discontinuation of prophylactic medication because of the pregnancy. Studies show that even with a his to ry of bipolar affective illness, a relapse of the illness tends not to occur during pregnancy (Marks et al. There are also case reports which show that patients with severe bipolar illness improved significantly during pregnancy (Sharma and Persad 1995). Angst (eds), Bipolar Disorders: 100 years after manic-depressive insanity, 127�137. Before the frequency of bipolar disorders in the post-partum period is discussed we define the three most important psychiatric post-partum disturbances: 1. The most frequently reported disturbance (found in 50�70% of all deliv eries) is the postnatal blues or baby blues which occur between the third and fifth day after delivery. Baby blues can be classified as a "physio logical" consequence of the very abrupt hormonal changes after deliv ery. Post-partum depression ranging from very mild respectively minor depression to major depression with psychotic symp to ms, is more fre quently reported (found in approximately 10�15% of all deliveries) and, in most cases, occurs within the first weeks or months after delivery. Post-partum psychosis starts in the majority of cases within the first 2 weeks post partum in approximately one or two of every 1000 deliver ies (Brocking to n and Cox-Roper 1988, Gitlin and Pasnau 1989, Kendell et al. When the frequency of these different types of disorders is calculated on the basis of approximately 800 000 deliveries per year in Germany, it becomes clear that compared to post-partum depression, post-partum psy chosis is only a "minor" problem with regard to the to tal number of cases (see Figure 1). Especially in regard to post-partum depression, it is well established that, in the majority of cases, psychological and social fac to rs (for example, personality, role expectations, etc. Here, especially, the interaction between oestrogen and the sero to nin system is discussed. Here, the question of hypersensitivity of dopamine recep to rs is one of the targets of studies in that field (Wieck et al. Nevertheless, that psychological aspects may also have some influence can be shown by the fact that also "bipolar fathers" also have relapses of illness when their wives become pregnant and have children (Davenport 1982). It is currently believed that affective disorders and post-partum psychoses have a multifac to rial aetiology, and hormonal changes are only one of these fac to rs. Also important are, among others, genetic disposition, sociobio graphical parameters and psychological stress. It was discovered that for women with a his to ry of manic depressive illness, manic or depressive, the risk of psychiatric admission in the puerperium was much higher than for those women with a his to ry of schizophrenia or depressive neurosis. Within the first 30 days after child birth the risk for psychiatric admissions was found to be 21. Linking the Danish Medical Birth Register and the Danish Psychiatric Central Register, Terp and Mortensen (1998) found that although childbirth is indeed a strong risk fac to r for a first admission with psychosis the risk in general may be less than previously assumed. Compared with unipolar affective disorders the risk for admission was about twice as high for bipolar patients, whether for first admissions or for readmissions. Indeed, in cases of women with bipolar affective disorders, hospital admission to ok place immediately after delivery with a relative risk of 2. Thus, a his to ry of a bipolar disorder is a strong risk fac to r in post-partum psychosis. Marneros Diagnostic categories of post-partum psychosis Emil Kraepelin, who also expressed his views on this to pic in his textbook of psychiatry, also deserves to be mentioned. It was his opinion that about 14% of all mental disorders in female inpatients in mental asylums were a consequence of gestational functions such as pregnancy, delivery or lacta tion (Kraepelin 1903). He also made clear that, in his view, "puerperal mania" � an often-used general term for post-partum disorders in the late 1800s/early 1900s. Fuerstner 1875) � is not a disease entity, but rather a group of illnesses that may occur post partum. This opinion is still valid, or, "valid again", after a number of studies that unsuccessfully sought to find support for the hypothesis that puerperal disorders are a separate nosological entity. Kraepelin saw mostly manic or cata to nic states of excitement, especially the latter, often during the course of dementia praecox and less frequently during infection delirium or exhaustion delirium (Kraepelin 1903) � an observation which is in accor dance with modern findings. Brocking to n and Kendell in England) who see manic or schizomanic illnesses as the main representation of psychotic disorders post partum (Brocking to n and Cox-Roper 1988, Kendell et al. But there are other research groups � including our own � that have additionally found a significant number of paranoid hallucina to ry schizophrenia, cata to nic schizophrenia or schizophreniform disorders (Rohde and Marneros 1993) resp. Bipolar post-partum disorders in the Cologne Study Some of the findings of the Cologne Study (a long-term study on schizo phrenic, schizoaffective and affective disorders, Marneros et al. Of a study population of 86 patients hospitalized between 1950 and 1979 because of a post-partum psychosis we were able to follow up on 61 patients and evaluate the whole course of their illness � on average 25.
Because of his abnormal cholesterol medication nz buy 20 mg atorvastatin mastercard, obsessional (anankastic) personality which cholesterol ratio is most important purchase line atorvastatin, he responded to cholesterol kit walmart order genuine atorvastatin on line the stress of promo tion by becoming acutely distressed and developing neurotic depressive symp to can cholesterol medication cause joint pain buy atorvastatin 20mg without a prescription ms. His psychopathic blunting of appreciation for the way others would experience his behaviour and their consequent feelings resulted in him causing suffering to others. Whether or not it manifests as personality disorder depends to a considerable extent on social circumstances. A highly abnor mal personality that in one situation may be considered criminal psychopathy and be possessed by a convicted prisoner, in another situation will be the driving force in a highly successful and relatively creative political revolutionary. Personality in an individual cannot be divorced from its social and cultural setting. Indeed, some have argued that the personality disorder constructs that we currently utilize are derived from and calibrated against Western middle-class cultural norms (Mulder, 2012). Having ascertained whether personality disorder is present, its type should be categorized using an accepted system. It is often extremely diffcult to ft people in to arbitrary categories of personality, and the whole to pic of classifcation is still highly unsatisfac to ry. It may be much better to use a few descriptive sentences for the personality, and probably it is best to combine description with categorization. They all start from the same bases: the defnition of personal ity, the evaluation of abnormality and the observation of certain infuential and regularly occurring traits. It is important to realize that these categories are not mutually exclusive: mixed personality types are more frequent than a single personality type in pure form. Readers in the United Kingdom or in countries infuenced by British psychiatry should be aware of an ongoing source of confusion perpetuated by recent discussion of the legal and administrative aspects concerning �dangerous people with severe personality disorder� (Haddock et al. In descriptive psychopathology, this debate is almost entirely concerned with dissocial personality disorder, but those taking part in the discussion tend to ignore other personality types, thus causing confusion for the assessment and classifcation of those with other personality disorders such as anankastic or anxious avoidant personality disorder. This can result in inappropriate treatment or lack of treatment being administered by mental health professionals and unjustifable stigmatization being experienced by the sufferers. Paranoid Personality Disorder the essential feature of this type of personality disorder is self-reference, the proper psychiatric sense of the word paranoid; such people misinterpret the words and actions of others as having special signifcance for, and being directed against, themselves. Theoretically, self-referent ideas could imply that others are always noticing them in an admiring and benevolent way; in practice, such people would not consult a psychiatrist and those presenting in psychiatry have ideas of persecution. They mistrust other people and are very sensitive and suspicious, believing that others are against them and that what they say about them is deroga to ry. There are active and passive types of paranoid personality disorder; both types feel that others are �getting at them� but their response differs. The active paranoid personality manifests suspiciousness and is hostile and untrusting. Such a person is quarrelsome, litigious, quick to take offence, intensely suspicious and sometimes violent; he will go to enormous lengths to defend his rights or to address real or imagined injus tices. He is extremely vigilant and tenacious in taking precautions against any perceived threat. They repudi ate blame and may be regarded by others as devious, scheming and secretive. Such a person is intensely jealous of what he regards as his own belongings, which may be people as well as objects, and he spends a lot of time planning to �get his own back�. Morbid jealousy may be shown, and such a person may be involved in acts of violence because of imagined injustice. Such a personality may fnd creative expression in social and political life but is likely to be very destructive within the family. A patient commented on this ruefully, �I have scarcely talked to my wife for the last ten years�, because of his succession of court cases against those with whom he came in to contact. A person with passive paranoid personality faces the world from a position of submission and humiliation. Like the active type, he is suspicious, sensitive and self-referent and misconstrues circumstances and other people. He believes that other people will dislike him and that they will ultimately let him down. However, he accepts �the slings and arrows of outrageous fortune� passively, bowing to the inevitable; he is vulnerable and frequently feels humiliated and unable to initiate any assertive activity. Other people tend to take advantage of him, thus fulflling his pessimistic expectations. A frequent manifestation of psychopathology within the context of paranoid personality is the presence of an overvalued idea (Chapter 8). This, alternatively described as a fxed idea (idee fxe), is a belief that might seem reasonable both to the patient and to other people. However, it comes to completely dominate the person�s thinking and life, and instead of testing its validity he tends to consider that every circumstance of life substantiates it; it becomes the basis for action that is sometimes aggressive or self-destructive. Schizoid Personality Disorder this personality disorder is characterized by a lack of need for, and defect in, the capacity to form social relationships. Such people show withdrawal from social involvement; emotional cool ness and detachment; and indifference to the praise, criticism and feelings of other people. These individuals are �loners� with a disinclination to mix, and they appear somewhat aloof. They lack tender feelings, have little interest in sexual experience and are not interested in the company of others. They are not depressed in mood, nor are they shy or sensitive to wards other people, but they are solitary and prefer not to be involved in social occupations. Their interests and hobbies usually tend to increase their isolation from other people, as they are more interested in things, objects and machines. Close relatives may complain of the subject�s emotional detachment, an inability to inspire strong feelings in others, a lack of any real sense of pleasure, oddness and eccentricity and callous indifference to others� suffering. In a follow-up of former schizoid subjects, they were found to use psychological constructs less than a control group, and this pointed to the schizoid individual�s lack of empathy (Chick et al. Those with schizoid personality and poor social adjustment have been considered more likely to develop schizophrenia. In a large study based on the previous personality assessment of 50,054 male recruits to the Swedish army, aspects of personality were found to be risk fac to rs for the subsequent development of schizophrenia (Malmberg et al. Dissocial Personality Disorder the essential, phenomenological abnormality of dissocial (asocial, antisocial or psychopathic) personality disorder is primarily one of empathy. This personality type, or abnormality, includes those people consid ered to suffer from psychopathic personality within the meaning of the Mental Health Act, 1983 (Bluglass, 1983). A normal person is prevented most of the time, by shame or by his capacity for empathy, from carrying out unpleasant actions to wards other people. He does not want to be disliked and feels very keenly how it would be passively to be the recipient of such behaviour. It is this inability to feel for himself the discomfort that others experience as a result of his antisocial activities that appears to be absent in the psychopath. Despite such comprehensive descriptions as that of Cleckley (1941), in the Mask of Sanity, and others, there are still considerable doubts as to whether this personality type forms a distinct category or not, and if it does, whether it should be considered within or outside psychiatry. This is succinctly expressed by Woo to n (1959): psychopaths are �extremely selfsh persons and no one knows what makes them so�. The confusion of terminology is explained partly by the varied nature of presentation; partly by the conficting desires of professionals not to stigmatize and also not to cast blame on those who cannot control their actions; and partly by the requirements of classifcation for different professional groups and settings � lawyers, criminologists, psychiatrists, psychologists and so on. A comprehensive account of diagnostic issues, developmental his to ry and methods of treatment is to be found in Dolan and Coid (1993). The concept of moral derangement was introduced by Benjamin Rush (1812), and of moral insanity by Prichard (1835), who considered this to occur among criminals who showed loss of feeling, of control, and of ethical sense, equivalent to mental disease but at a different level. It is important to stress that not all psychopaths are criminal, nor are all criminals psychopathic. Henderson (1939) described creative, inadequate and aggressive psychopathy, citing Lawrence of Arabia as an example of a creative psychopath. Dissocial personality disorder, with conspicuous lack of conscience and human sympathy, is found more often in males than in females. This personality disorder should not be diagnosed unless the subject is aged over 18 years.
Atorvastatin 40 mg with mastercard. കൊളസ്ട്രോൾ എളുപ്പം നിയന്ത്രിക്കാം | Cholesterol Malayalam Health Tips.
Aims of Treatment Planning the overarching aims of treatment planning are severalfold: 1) to cholesterol levels paleo diet atorvastatin 5mg mastercard promote and maintain recovery cholesterol in foods list generic atorvastatin 40mg overnight delivery, 2) to p-cholesterol-ratio buy atorvastatin master card maximize quality of life and adaptive functioning cholesterol ratio the lower the better cheap atorvastatin on line, and 3) to reduce or eliminate symp to ms. To achieve these aims, it is crucial to identify the patient�s aspirations, goals for treatment, and treatment-related preferences. Depending on prevailing state laws, psychiatric advance directives are one approach to encouraging patients to contemplate and state their preferences about treatment choices (Easter et al. For patients who have completed a psychiatric advance directive, wellness recovery action plan (Copeland 2000), or individualized crisis prevention or safety plan (Safety Planning Intervention 2018; Stanley and Brown 2012; Stanley et al. The patient and others may express opinions about specific treatment approaches or identify practical barriers to the patient�s ability to participate in treatment, such as lack of insight, cognitive impairments, disorganization, or inadequate social resources. Elements of the Treatment Plan Depending on the clinical circumstances and input from the patient and others, a comprehensive and person-centered treatment plan will typically delineate treatments aimed at improving functioning, reducing positive and negative symp to ms, and addressing co-occurring psychiatric symp to ms or disorders. In each of these respects, it is essential to consider both nonpharmacological and pharmacological treatment approaches and recognize that a combination of nonpharmacological and pharmacological treatments will likely be needed to optimize outcomes. Most individuals welcome involvement of family members and other persons of support (Cohen et al. Family members can also be provided with educational materials or directed to organizations that offer education to family members and other persons of support (National Alliance on Mental Illness 2019; Mental Health America 2019). Strategies to Promote Adherence Strategies to promote adherence are always important to consider in developing a patient-centered treatment plan (Ferrando et al. Treatment planning to address adherence will depend on the specific contributing fac to rs and whether reduced adherence is related to medication use, missed appointments, or other aspects of treatment. Issues that may influence adherence include, but are not limited to, lack of awareness of illness, forgetting to take doses, difficulties managing complex regimens. Adherence with appointments can also be influenced by financial barriers, difficulties scheduling visits around work or school schedules, or issues with transportation or with childcare. In assessing adherence, it is important to take a patient-centered approach in inquiring in a non judgmental way whether the individual has experienced difficulties with taking medication (Haddad et al. Obtaining information from patient diaries, patient-completed rating scales, pharmacy records, family members, or other collateral sources of information can be useful supplements to subjective patient reporting (Acosta et al. Tablet counts, moni to ring using electronic pill bottle caps, and drug formulations with implanted sensors have also been used to assess adherence with antipsychotic medications (Acosta et al. Levels of clozapine have been best studied but blood levels of other antipsychotic medications are also available. Although the utility of routine therapeutic moni to ring is unclear for antipsychotic medications other than clozapine, blood levels may help in establishing whether a patient is taking the medication (Hiemke et al. Urine levels of antipsychotic medications can also be used to assess for adherence (Velligan et al. However, evidence on the most effective techniques remains limited (Hartung et al. A checklist that includes barriers, facilita to rs, and motiva to rs for adherence has been developed and may be helpful in promoting discussion and identifying adherence related fac to rs in individual patients (Pyne et al. In addition to conducting ongoing moni to ring of adherence as treatment proceeds, it can be helpful to focus on optimizing treatment efficacy, addressing side effects and concerns about treatment, adjusting dosing to minimize side effects while maintaining efficacy, providing information about the illness and its treatments, engaging in shared decision-making, fostering a strong therapeutic alliance, and engaging family members and other community and social supports, as appropriate (Acosta et al. For some patients, the formulation of the antipsychotic medication may influence adherence (see Table 3, Statement 4). If financial issues with medications are affecting adherence, reassessment of the treatment regimen may be needed or patients� assistance programs may be pursued. When a patient does not appear for appointments or 42 is nonadherent in other ways, assertive outreach such as telephone calls or secure messages, may be helpful in reengaging the patient in treatment. Addressing Risks for Suicidal and Aggressive Behavior Identifying risk fac to rs and estimating risks for suicidal and aggressive behaviors are essential parts of psychiatric evaluation (American Psychiatric Association 2016a and as described in detail in the Implementation section of Statement 1 of this guideline). Despite identification of these risk fac to rs, it is not possible to predict whether an individual patient will engage in aggressive behaviors or attempt or die by suicide. However, when an increased risk for such behaviors is present, it is important that the treatment plan re-evaluate the setting of care and implement approaches to target and reduce modifiable risk fac to rs. Although demographic and his to rical risk fac to rs are static, potentially modifiable risk fac to rs may include poor adherence, core symp to ms of schizophrenia. Additional elements of the treatment plan can address periods of increased risk. Addressing Tobacco Use and Other Substance Use Disorders Individuals with schizophrenia have high rates of nicotine dependence (Centers for Disease Control and Prevention 2019b; Cook et al. Smoking is a major contribu to r to increased mortality in individuals with serious mental illness (Reynolds et al. Some studies have assessed smoking cessation approaches targeted to individuals with mental illnesses, but specific evidence in patients with schizophrenia is still limited (Sharma et al. Although quit rates may be lower in individuals with schizophrenia than in the general population (Lum et al. Rates of cannabis use and other substance use are also increased among individuals with schizophrenia (Hartz et al. Other substance use disorders are associated with a poorer prognosis in individuals with schizophrenia (Brunette et al. Thus, it is important for the treatment plan to address substance use disorders when they are present. Often, a comprehensive integrated treatment model is suggested in which the same clinicians or team of clinicians provide treatment for schizophrenia as well as treatment of substance use disorders. However, if an integrated treatment is unavailable, the treatment plan should address both disorders with communication and collaboration among treating clinicians. For patients who do not recognize the need for treatment of a substance use disorder, a stage-wise motivational approach can be pursued (Catley et al. Addressing Other Concomitant Psychiatric Symp to ms and Diagnoses Depressive symp to ms are common in individuals with schizophrenia and should be addressed as part of treatment planning. The approach to treating depression will be grounded in a careful differential diagnosis that considers the possible contributions of demoralization, negative symp to ms of schizophrenia, side effects of antipsychotic medications, substance in to xication or withdrawal, physical health condition, or a co-occurring major depressive episode. Depressive symp to ms that occur during an acute episode of psychosis often improve as psychotic symp to ms respond to treatment. Evidence on the use of antidepressants to treat depression in individuals with schizophrenia comes from multiple trials, many of which have small sample sizes or fac to rs that increase the risk of bias in the findings (Donde et al. Nevertheless, meta-analysis suggests that the addition of antidepressant medications results in small beneficial effects on symp to ms of depression, quality of life, and response rates as well as on positive symp to ms, negative symp to ms, and overall symp to ms (Helfer et al. These effects were more prominent in patients with more severe depressive symp to ms. Furthermore, antidepressant treatment did not appear to be associated with exacerbation of psychosis or significant differences in adverse effects (Helfer et al. Non-pharmacological treatments for depression in schizophrenia have been less well studied but could also be incorporated in to treatment planning (Donde et al. Nevertheless, many individuals with schizophrenia will have experienced violent victimization (de Vries et al. When anxiety symp to ms are present in individuals with schizophrenia, the possible contributions of psychotic symp to ms, medication side effects, substance in to xication or withdrawal, or co-occurring anxiety disorders may suggest an approach to treatment. Given the relative safety of adjunctive antidepressant medications in individuals with schizophrenia and depression, these medications may be considered if otherwise indicated to treat posttraumatic stress disorder or an anxiety disorder. On the other hand, studies on the use of benzodiazepines in schizophrenia are limited (Dold et al. Non-pharmacological treatments for posttraumatic stress disorder in individuals with schizophrenia have been less well studied but may have modest benefits and do not appear to have significant adverse effects as compared to usual care (Brand et al. In terms of the use of stimulants to treat pre-existing attention-deficit/hyperactivity disorder in individuals with schizophrenia, available evidence is also very limited but suggests a potential for worsening of psychotic symp to ms as well as potential for development of a stimulant use disorder (Sara et al. Thus, if stimulant medications are used, moni to ring for these possible adverse effects is warranted as part of the treatment plan. Addressing Other Concomitant Health Conditions As described in Statement 1, other health conditions are more frequent in individuals with serious mental illness in general (Firth et al. Impairments in renal and hepatic function, if present, can influence treatment recommendations. Table 2 of Statement 1 provides a discussion of suggested physical and labora to ry assessments for patients with schizophrenia as part of initial evaluation and follow-up assessments.
Based on the age effects estimated from several reviews and studies cholesterol over 200 cheap atorvastatin 40 mg amex, an unhappy person � 2011 the Authors is cholesterol in shrimp bad for you buy atorvastatin 40mg mastercard. This variability is clearly demonstrated in a study on the effects of smoking (Doll cholesterol vitamin d atorvastatin 20 mg online, Pe to cholesterol medication gemfibrozil purchase generic atorvastatin on line, Wheatley, Gray, & Sutherland, 1994), in which British physicians were assessed over a period of 40 years. Death rates due to smoking were double in the second 20 years compared to the first 20 years. Had the investiga to rs followed partici pants for 10 years and controlled for initial health at the start of the study, the effects would have been much smaller. Thus, the effects found in studies rarely give the full lifelong effects of lifestyle and personality fac to rs. Operating in the opposite direction is that for the majority of past studies in this field positive feelings were not assessed. Segerstrom & Miller, 2004; Herbert & Cohen, 1993) have analyzed the distributions of research findings, and concluded that publication bias is unlikely to produce the full effects found, although it might have some effect. In some analyses no evidence of publication bias has been discovered, and in others researchers have found likely publication bias, but also that an extremely large number of unreported studies would be required to reverse the findings. Given the unsettled nature of this area, it seems unlikely that huge numbers of negative findings are unreported. Indeed, one could imagine situations in which meth odologies that would be considered adequate in other areas of study would be considered inadequate in this area, resulting in a negative edi to rial bias. However, as evidence accumulated, much of the skepticism narrowed to more specific questions. Coyne and Tennen (2010; Coyne, Tennen, & Ranchor, 2010) concluded that evidence is lacking that a �fighting spirit� or �benefit finding� slow cancer progression. A decade ago skepticism that hostility could increase the likelihood of heart disease was expressed. Myrtek, 2001; Petticrew, Gilbody, & Sheldon, 1999), but more recent reviews have concluded that the case for the link is compelling (Smith et al. Thus, over time skepticism has focused on the open questions that have not yet been answered in a clear and con vincing way. Bjornskov (2008) expressed new skepticism about the benefits of happiness for health. He suggested that society-wide happiness might decrease longevity because happy societies spend less on public health. In a sample of 15 eco nomically developed European Union nations he found that the average life satisfaction in the societies negatively predicted their public health expendi tures. Following up on this suggestion in 95 diverse nations included in the Gallup World Poll, we found the opposite of what Bjornskov found in his small and homogeneous sample of nations. We will report these findings in detail in a later paper, but it appears to us that happy nations do not spend less on health or have shorter life expectancy. High subjective well-being is a state that many desire, some achieve, and a few despise as an unnecessary luxury or even a detriment. Koivumaa-Honkanen, Howard Friedman, Howard Tennen, Janice Kiecolt-Glaser, John Helliwell, Sonja Lyubomirsky, Karen Matthews, Kyriakos Markides, Laura Kubzansky, Michael Frisch, Richard Eckersley, Robert Biswas-Diener, Robert Cummins, Ruut Veenhoven, Ryan Howell, Sarah Pressman, Suzanne Seger strom, William Pavot, and Rosemarie Kobau. Our thanks to the Robert Wood Johnson Foundation and the John Temple to n Foundation for support that helped make the writing of this paper possible. Larger effect sizes were associated with higher quality ratings in complementary and alternative medicine randomized controlled trials. Lower myocardial infarction mortality in French men the day France won the 1998 World Cup of football. Suicide rates, life satisfaction and happiness as markers for population mental health. Positive affect is associated with cardiovascular reactivity, norepinephrine level, and morning rise in salivary cortisol. Ratings of positive and depressive emotion as predic to rs of mortality in coronary patients. Prediction of all-cause mortality by the Minnesota Multiphasic Personality Inven to ry Optimism-Pessimism Scale scores: Study of a college sample during a 40-year follow-up period. Stress reduces conception probabilities across the fertile window: Evidence in support of relaxation. The effects of social status on biological aging as measured by white-blood-cell telomere length. Positive psychological well-being and mortality: A quantitative review of prospective observational studies. Chronic social stress, affiliation, and cellular immune response in nonhuman primates. Positive psychology in cancer care: Bad science, exaggerated claims, and unproven medicine. Accelerated telomere erosion is associated with a declining immune function of caregivers of Alzheimer�s disease patients. Individual differences in prefrontal activation asymmetry predict natural killer cell activity at rest and in response to challenge. Don�t worry, be happy: Positive affect and reduced 10-year incident coronary heart disease: the Canadian Nova Scotia Health Survey. Effects of attention and rewarded activity on immune parameters and wound healing in pigs. Social support and positive affect as predic to rs of pain sensitivity in fibromyalgia and control participants (Doc to ral dissertation). Dissertation Abstracts International: Section B: the Sciences and Engineering, 69(7�B), 4474. Health risk reduction and functional res to ration following coronary revascularization: A prospective inves tigation using dynamic stage typology clustering. Elderly patients with hip fracture with positive affect have better functional recov ery over 2 years. Positive emotions speed recovery from the cardiovascular sequelae of negative emotions. Expressions of positive emotion in pho to graphs, personality, and later-life marital and health outcomes. Psychosocial and behavioral predic to rs of longevity: the aging and death of the �Termites�. Alteration of type A behavior and its effect on cardiac recurrences in post myocardial infarction patients: Summary results of the recurrent coronary preven tion project. The short-term effects of a hostility reduction intervention on male coronary heart disease patients. Dispositional optimism and all-cause and cardiovascular mortality in a � 2011 the Authors. The relationship between life satisfaction and health behavior: A cross-cultural analysis of young adults. A longitudinal assessment of breast, colon, and lung cancer patients (Doc to ral dis sertation). Dissertation Abstracts International: Section B: the Sciences and Engi neering, 57(6�B), 4029. Psychosocial fac to rs in the aetiology and prognosis of coronary heart disease: Systematic review of prospective cohort studies. Health benefits: Meta analytically determining the impact of well-being on objective health outcomes. Promoting and protecting mental health as fiourishing: A complementary strategy for improving national mental health. Hostile marital interactions, proinfiamma to ry cy to k ine production, and wound healing. Mental health promotion in public health: Perspectives and strat egies from positive psychology. Exercise and psychosocial fac to rs modulate immunity to infiuenza vaccine in elderly individuals. Effects of happiness on all-cause mortality during 15 years of follow-up: the Arnhem Elderly Study. A prospective study of optimism and coronary heart disease in the normative aging study.