

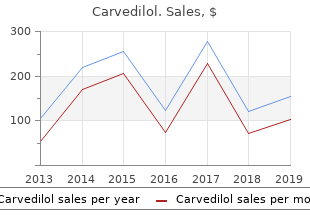
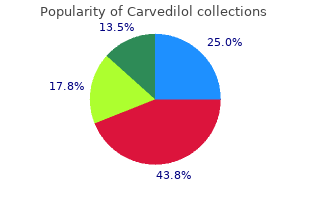
Carvedilol
"Discount carvedilol 12.5mg, blood pressure problems."
By: Paul Reynolds, PharmD, BCPS
- Critical Care Pharmacy Specialist, University of Colorado Hospital
- Clinical Assistant Professor, Department of Clinical Pharmacy, Skaggs School of Pharmacy and Pharmaceutical Sciences, University of Colorado, Aurora, Colorado

http://www.ucdenver.edu/academics/colleges/pharmacy/Departments/ClinicalPharmacy/DOCPFaculty/Q-Z/Pages/Paul-Reynolds,-PharmD.aspx
However heart attack diet purchase carvedilol cheap online, even in agoraphobia without history of panic disorder blood pressure medication guidelines buy genuine carvedilol on-line, agoraphobia is considered related to heart attack telugu movie buy discount carvedilol 12.5mg online the fear of developing paniclike symptoms hypertension treatment guidelines jnc 7 buy carvedilol mastercard. These include specific and social phobia, generalized anxiety disorder, and major depressive disorder. Some data also suggest associations with substance use disorders, bipolar disorder, and suicidal behavior. While the high comorbidity seen in the clinic partially reflects referral bias, considerable comorbidity with these anxiety and depressive disorders is also found in epidemiological studies, which suggests that panic disorder in the community is frequently compounded by comorbid mental conditions. Between 1980 and 1994 one significant change to the conceptualization of the disorder involved refining the view of panic disorder and agoraphobia as tightly linked constructs. Panic attacks are associated with a variety of endocrinological disorders, including both hypo and hyperthyroid states, hyperparathyroidism, and pheochromocytomas. Episodic hypoglycemia associated with insulinomas can also produce paniclike states, as can primary neuropathological processes. These include seizure disorders, vestibular dysfunction, neoplasms, or the effects of both prescribed and illicit substances on the central nervous system. Finally, disorders of the cardiac and pulmonary systems, including arrhythmias, chronic obstructive pulmonary disease, and asthma, can produce autonomic symptoms and accompanying crescendo anxiety that can be difficult to distinguish from panic disorder. Clues of an underlying medical cause for paniclike symptoms include atypical features during panic attacks, such as ataxia, alterations in consciousness, or bladder dyscontrol; onset of panic disorder relatively late in life; or physical signs or symptoms indicating a medical disorder. Panic disorder also must be differentiated from a number of psychiatric disorders, particularly other anxiety disorders. Since panic attacks occur in many anxiety disorders, including social and specific phobia, posttraumatic stress disorders, or even obsessive-compulsive disorder, the key to correctly diagnosing panic disorder involves documenting recurrent spontaneous panic attacks at some point in the illness. Classically, panic attacks are characterized by their rapid onset, within minutes, and short duration, usually less than 10 to 15 minutes, in contrast to the anxiety associated with generalized anxiety disorder, which emerges and dissipates more slowly. This distinction can be difficult, however, as the anxiety surrounding panic attacks can be more diffuse and dissipate more slowly. Since anxiety is a frequent concomitant of many other psychiatric disorders, including the psychoses and affective disorders, distinctions between panic disorder and a multitude of disorders can also be difficult. Course Panic disorder typically has its onset in late adolescence or early adulthood, although cases of childhood-onset and late adulthood�onset disorder have been described. The best evidence on the course of any disorder, including panic disorder, derives from prospective epidemiological research, since both retrospective and clinically based studies are vulnerable to biases that preclude firm conclusions on course. Retrospective or clinical studies suggest that panic disorder tends to exhibit a fluctuating course, with varying levels of persistence over the life span. Approximately one third to one half of patients are psychiatrically healthy at follow-up, with most living relatively normal lives, despite either fluctuating or recurrent symptoms. Typically, patients with chronic disorders exhibit a pattern of exacerbation and remissions rather than chronic disability. Her first visit was prompted by a paroxysm of extreme dyspnea and terror that occurred while she was working on a term paper. The dyspnea was accompanied by palpitations, choking sensations, sweating, shakiness, and a strong urge to flee. She developed two other similar episodes, one while she was on her way to visit a friend and a second that woke her up from sleep. She immediately went to the emergency room after experiencing both paroxysms, receiving full medical workups that showed no sign of illness. Both specific and social phobia require the development of intense anxiety, to the point of even situationally bound panic, upon exposure to the feared object or situation. Both conditions also require that fear either interferes with functioning or causes marked distress. Finally, both conditions require that an individual recognizes the fear as excessive or irrational and that the feared object or situation is either avoided or endured with great difficulty. The key feature in each type of phobia is that the fear is circumscribed to a specific object, both temporally and with respect to other objects. Hence, an individual with specific phobia becomes immediately frightened when presented with a feared object. This fear may relate to concern about harm from a feared object, concern about embarrassment, or fear of consequences related to exposure to the feared object. For example, individuals with blood-injury phobia may be afraid of fainting on exposure to blood, and individuals with fear of heights may be afraid of becoming dizzy. Specific phobia often involves fears of more than one object, particularly within a specific subcategory of phobia. For example, it is common for an individual with a phobia of thunderstorms to also have a phobia of water, both phobias being classified as natural environment type phobias. Further, in the clinical setting, specific phobia often occurs with other anxiety or mood disorders. Since it is rare for patients to seek treatment for an isolated phobia, some of the comorbidity seen in the clinic reflects referral bias. Community-based studies also suggest that specific phobia is associated with other anxiety disorders, although at lower rates than seen in the clinic. Quantifying the impairment associated with a specific phobia is sometimes difficult, since the comorbid disorders typically tend to cause more impairment than specific phobia and since individuals with isolated specific phobia are rarely seen in the clinic. Impairment associated with specific phobia typically restricts the social or professional activities of the individual. Social phobia involves fear of social situations, including situations that involve scrutiny or contact with strangers. Individuals with social phobia typically fear embarrassing themselves in social situations. This can involve specific fears about performing certain activities, such as writing, eating, or speaking in front of others. Individuals with social phobia who fear most situations are considered to suffer from generalized social phobia. Such individuals are fearful of initiating conversations in many situations, about dating or participating in most group activities or social gatherings, and about speaking with authority figures. The clinician should recognize that many patients exhibit at least some social anxiety or self consciousness. In fact, community studies suggest that roughly a third of all people consider themselves to be far more anxious than other people in social situations. Such anxiety only becomes social phobia when the anxiety either prevents an individual from participating in desired activities or causes marked distress in such activities. Individuals with the more specific form of social phobia possess fear of specific, circumscribed social situations. As with other anxiety disorders, social phobia frequently co-occurs with other mood and anxiety disorders. The association of social phobia with both panic disorder and major depression has received considerable attention in recent literature. Associations with substance use disorders and childhood conduct problems have also been documented. History and Comparative Nosology Phobias have been recognized as incapacitating mental disorders for more than 100 years. The prominent place of phobia in the history of modern mental health science is indicated by the major role case histories of phobic patients played in the development of both psychoanalytic and cognitive therapies. The category of phobia has undergone progressive refinement over the past 20 years, as research has focused on each of the specific classes of phobia described above. This change was based on descriptive phenomenology, epidemiology, and pharmacology studies that validated the two variants of the condition. Differential Diagnosis Specific phobia is usually quite easily distinguished from anxiety stemming from primary medical problems by the focused nature of the anxiety, which is not typical of anxiety disorders related to medical problems. The most difficult diagnostic issues involve differentiating specific phobia from other anxiety disorder. Similarly, specific phobia can occasionally be confused with generalized anxiety disorder, as both conditions may involve worry about exposure to specific situations. The two disorders are differentiated on the basis of the focused nature of the fear, both over time and with respect to objects, in specific phobia. Like specific phobia, social phobia is rarely confused with anxiety that is the primary result of medical disorders. However, the number of psychiatric disorders that are associated with social withdrawal make it difficult to diagnose social phobia correctly. Perhaps the most difficult distinction involves differentiating social phobia and agoraphobia, since both conditions involve fears of situations where people typically gather. The key distinction between the disorders centers on the nature of the feared object.
Vascular Rings Yet another cause of stridor in children is vascular rings 18 order carvedilol 12.5mg without a prescription, which may also be accompanied by periods of apnea pulse pressure equivalent purchase 12.5 mg carvedilol. Compression of the trachea is 128 caused by either the innominate artery or any number of mediastinal vas cular rings that can occur embryologically hypertension drug list cheap carvedilol 6.25 mg online. For example hypertension 2014 order 6.25mg carvedilol fast delivery, a double-arched aorta may compress both the esophagus and the trachea. This diagnosis is generally made by visualizing an anterior compression of the trachea on bronchoscopy. A barium swallow will occasionally show an indentation behind the esophagus if there is a complete vascular ring present that encircles the esophagus and the trachea. If the symptoms are severe enough, treatment can include ligation and division of the ofending vessel or rerouting. Laryngomalacia The most common cause of persistent stridor in infants is laryngomala cia. Classically, this is associated with foppy supraglottic structures and an omega-shaped epiglottis. The noise is thought to be due to high-speed air fow through the narrow, redundant tissue of the supraglottic area. The diagnosis is established by fexible laryngoscopy performed at bedside, but synchronous lesions of the airway have been reported in up to 20 percent of patients. Some otolaryngologists advocate complete bronchoscopic evaluation of the airway to evaluate for these additional lesions. If there is no history of respiratory distress (apnea, cyanosis, retractions) and the patient is gaining weight well, treatment is simply observation, because these children will usually grow out of the condition. If the patient has apneic episodes or desaturates, then the supraglottic tissues can be trimmed or a tracheostomy can be performed. Other indications for surgi cal intervention include poor weight gain or failure to thrive. Congenital Neck Masses One of the common congenital neck masses is a lymphatic malformation, also known as a lymphangioma or cys 129 tic hygroma. Tese patients may need Neck masses arising in children are usually immediate intubation or a surgical air benign (as opposed to adults, in whom way at birth if the neck mass is large they are usually malignant). Tese are characteristically found along the anterior border of the sternocleidomastoid muscle. The cyst can occasionally become infected and swell, only to respond to antibiotic therapy, shrink, and then recur. Treatment is surgical excision with a Sistrunk operation, where the mid portion of the hyoid bone is removed along with the cyst�s stalk to the base of the tongue. Infectious Neck Masses Infectious causes of neck masses in children are more common than con genital causes. Perhaps the most common reason for enlarged lymph nodes in a child is tonsillitis or pharyngitis. Occasionally, the lymph nodes them selves can become infected, usually with Staphylococcus or Streptococcus species (cervical adenitis). You should always consider cat-scratch disease or atypical mycobacterial infection, when children present with suppurative adenitis without associated constitutional symptoms (fever, malaise, and The patient�s history of being scratched by a kitten is the key to making the diagnosis in cat-scratch disease. Atypical mycobacterial infection is occasionally a cause of swollen lymph nodes in children. Excision of the lymph nodes is indicated if they do not respond to medical therapy. This is essentially a cervical adenitis that occurs in the space behind the pharynx. Tese patients may have an obvious amount of infammation on the anterior spinal ligament, as well as up around the base of the skull, and can therefore present with a stif neck (meningismus) and fever. A sof-tissue lateral neck x-ray will usually show an increased thickness of the retropharyngeal space anterior to the spine. Cellulitis will respond to antibiotics, but abscesses frequently require surgical incision and drain age, through either the mouth or the neck. Vancomycin should be considered if resis tant organisms, such as penicillin-resistant S. Malignant Neck Masses Malignant neck masses in children are rare, and include salivary gland malignancy, which is treated surgically. Tumors of the thyroid gland also occur, and may be accompanied by metastatic disease in the lymph nodes. This can be either a dermoid cyst or a congenital herniation of the intracranial tissues (encephalo cele or meningoencephalocele). Tese patients should be referred for surgical excision, along with neurosurgical consultation as indicated. This makes it especially hard to make certain sounds like �L� (and to eat an ice cream cone), but is easily corrected by incising the frenulum. Rhinosinusitis All children (and adults) sufer from an occasional bout of rhinosinusitis. Parents, however, can demand antibiotic treatment because of the nasal drainage (ofen green, yellow, or gray), and when they cannot leave their sick child in daycare. It is important to reassure parents that these episodes are normal, and to resist the temptation to treat mucus with antibiotics. Some children, however, will have persistent illness that lasts for weeks or months and is associated with fever. Also, some children will ben eft from adenoidectomy, and occasionally sinus aspiration or even sur gery may be required. If an abscess develops with visual change, proptosis, or loss of normal eye movement, urgent surgical drainage is required to prevent loss of vision. Tese abscesses can ofen be drained successfully through an endoscopic approach, but an external incision (just medial to the medial canthus) may be required. Four indications for performing tonsillectomy are, and. The fuid has been present in his ears for three months, despite treatment with a three-week course of trimethoprim and sulfamethoxazole. Unilateral, foul-smelling rhinorrhea in a child is most commonly due 132 to a. A four-year-old girl presents at the emergency room with inspiratory stridor and a fever of 103�F, and she is drooling and leaning forward. Her mother states that the child was well four hours ago, and she thinks that the child swallowed a stick because her throat hurts now and she was playing with small sticks in the yard outside. You then call the anesthesiologist and pediatrician, but while waiting for them to arrive, you notice that the child is starting to tire out. In fact, she becomes so tired from trying to breathe that she simply faints and ceases all attempts at respiration. Your next patient in the emergency room is a one-year-old boy who presents with a chief complaint of stridor. On examination, he is not sitting up or leaning forward, and he is not drooling, but he has biphasic stridor. You therefore obtain a sof-tissue x-ray of the neck and a chest x-ray to look for the classic steeple sign. You are surprised when you fnd the child has actually aspirated a small metal object that appears to be the tip of a pen. A multiloculated cystic neck mass in a newborn child that transil luminates is most probably a. A midline neck mass in a child that moves when the child sticks out his tongue, but is otherwise not tender and is found in the area of the hyoid bone, is most probably a. A two-year-old child presents to you with a high fever and large, painful, and infamed lef posterior triangle lymph nodes. Another two-year-old child presents without fever and with no pain, but with large, frm lymph nodes in the posterior triangle of the neck.
Buy carvedilol 6.25mg on-line. Exercise Your Way to Lower Blood Pressure.
The most frequent symptoms are nasal discharge hypertension with bradycardia carvedilol 6.25mg on-line, nasal obstruction blood pressure increase during exercise order discount carvedilol on line, sore or �scratchy� throat blood pressure ranges for elderly cheap 6.25mg carvedilol free shipping, headache prehypertension 23 years old buy carvedilol overnight, and cough. Hoarseness, loss of taste and smell, mild burning of the eyes, and a feeling of pressure in the ears or sinuses due to obstruction and/ or mucosal swelling may also occur. Differential diagnoses allergic rhinitis is usually accompanied by a watery rhinorrhoea and sore, streaming eyes. Non-allergic rhinitis would present with chronic nasal discharge, again of watery consistency. Paracetamol is the frst line choice; its anti-pyretic and analgesic properties will help to relieve symptoms. Vitamin C in large daily doses (more than 1g daily) may provide a modest beneft in terms of reducing the duration of cold symptoms. Topical nasal decongestants, for example, ephedrine, oxymetazoline, xylometazoline, have an immediate benefcial effect on reducing nasal stuffness. Oral decongestants, for example, pseudoephedrine, phenylpropanolamine, are not as immediately effective as topical preparations but do not cause rebound congestion on withdrawal. Echinacea: recent randomised controlled trials have shown no beneft in either adults or children. Zinc lozenges: there is no strong evidence of effcacy although interest has grown in zinc as a treatment for the common cold and many claims for its effectiveness have been made. Database of Systematic Reviews 2007, Issue 1 MeReC: the management of common infections in primary care Volume 17 Number 3 December 2006 40 Responding to Minor Ailments 3. Systemic symptoms include tiredness, fever, a pressure sensation in the head, and itchiness. Differential diagnoses persistent (perennial) allergic rhinitis, where symptoms occur all year round, is mainly due to house dust mite or domestic pets. Non-sedating antihistamines, eg loratadine, cetirizine and acrivastine, are more appropriate choices in these instances. Azelastine (Aller-eze) is licensed for sale for adults and children over the age of 5 years. Where rhinitis is the main symptom, intranasal corticosteroids should be the frst line choice as they are more effective than oral antihistamines in reducing total nasal symptoms particularly nasal congestion and sneezing and can also improve eye symptoms. Beclometasone, budesonide, futicasone and triamcinolone can all be sold to adults over the age of 18 years, for a maximum period of use of three months. Sodium cromoglicate is a mast cell stabiliser available as eye drops and nasal spray. Oral decongestants, such as pseudoephedrine, in combination with an oral antihistamine, have been shown to be effective at treating nasal congestion symptoms of hayfever. Homoeopathic treatment: some trials have found homoeopathic treatment to be better than placebo but further trials are needed. Special considerations: Pregnancy pregnancy often exacerbates rhinitis but care is needed in selection of drugs to relieve symptoms. Sports people stimulants, such as ephedrine, are not permitted for use by athletes. Go to the Drug-Free Sport website and obtain an advice card listing examples of permitted and prohibited substances in sport. Her asthma symptoms are no worse, there is no wheezing during the day, and you decide that the cough is as a result of post nasal drip caused by the cold. Case study 4 an 18 year old student, who is the daughter of one of your regular customers, visits your pharmacy. Many pharmacists have a favourite one or two � effectively their own personal formulary. Drowsiness is a signifcant side-effect with most of the older antihistamines although paradoxical stimulation may occur rarely, especially with high doses or in children and the elderly. Drowsiness may diminish after a few days of treatment and is considerably less of a problem with the newer antihistamines. The severity of pain perceived in response to any given stimulus is modulated by previous experience, cultural determinants, one�s own assessment of the meaning of the pain and the feeling of control which the subject has over the pain. It can vary from person to person and the severity is diffcult for other people to gauge. Pain can be caused by a variety of conditions and examples of these commonly seen in the pharmacy are headache, toothache, musculoskeletal pain and period pain. Treatment options the three main otc analgesic options are paracetamol, ibuprofen and aspirin. Few of the studies have compared the three compounds directly and the data suggest no marked differences in effcacy. Paracetamol is ineffective against infammation but all three are equally effective antipyretics. Due to the risk of overdose associated with paracetamol and aspirin, pack sizes are restricted for otc purchase. Patients should be reminded that many otc preparations contain paracetamol, for example, cold and fu preparations, and that the maximum daily dose must be adhered to. Paracetamol overdose leads to nausea, vomiting and eventually hepatic failure, which is often not apparent for four to six days. Paracetamol is the only option for patients with a history of hypersensitivity to aspirin or nsaiDs or active peptic ulceration. Patients receiving oral anticoagulants, methotrexate or thiazides are also best treated with paracetamol if an analgesic is required, in order to avoid dosage adjustments. Paracetamol is less irritant to the stomach and so is often preferred, particularly in the elderly. Higher doses of opioid analgesics are associated with a risk of dependence and misuse, either intentional or unintentional. Caffeine is a weak stimulant which, when included in analgesic preparations, is claimed to enhance the analgesic effect. Practical Tips there are various non-pharmacological measures that can be used to aid pain relief, depending on the cause: � heat, eg hot water bottle or a bath for muscular aches or period pain � cold compresses for headaches or sprains � massage to help relieve headaches or muscular pains � exercise for period pain or osteoarthritis 52 Responding to Minor Ailments 4. Usually the bottom front teeth erupt frst, followed by the top front teeth (central incisors) and then the top and bottom incisors on either side (lateral incisors). Treatment options Analgesia with paracetamol will be frst line treatment (babies over three months old). Parents should be advised to wash their hands thoroughly before applying topical agents directly to the mucous membrane. Homoeopathic remedies may be tried although there is no clinical evidence to support their use. Teetha teething Granules contain chamomilla at 6c potency, and advise that one sachet should be poured into the infant�s mouth every two hours, up to a maximum of six doses in 24 hours. Practical Tips a chilled teething ring may help to can also help but should be given soothe sore gums. Petroleum jelly or aqueous cream teething rings should not be tied applied around the mouth and chin around a baby�s neck. Muscle strains or �pulls� are most commonly caused by participating in sports which involve sprinting or jumping. Injury can be due to over-stretching the muscle or causing the muscle to contract too strongly. Differential diagnoses an inability to bear weight and bone tenderness suggests fracture may have occurred. Ice reduces pain; this can be done by immersing the affected part in ice water for up to 10 minutes, or applying a malleable ice-pack covered with a wet cloth (eg bag of frozen peas) for up to 15 minutes. Paracetamol and ibuprofen may be used together if one analgesic agent alone provides sub-optimal pain relief. Arnica gel is a traditional herbal medicinal product for the symptomatic relief of muscular aches, pains and stiffness, sprains, bruises and swelling after contusions. Published trials are methodologically weak and do not provide strong enough evidence to recommend its use. Patients were randomised to receive either high (30c) or low (6c) potency homoeopathic arnica or an indistinguishable placebo. Warm ups and stretching are early mobilisation of the injured area felt to be benefcial although there is is important, within the range of little good evidence to support this discomfort, so improving the range strategy. Special considerations: low back pain low back pain, defned as pain between the bottom of the ribs at the back and the top of the legs, is a common complaint in primary care.
Provoking an immune response in this way before a natural viral infection occurs acts to prehypertension bp range generic carvedilol 25mg �blueprint� immunologic memory so that cells involved in making the potential antiviral immune response are primed and held alert hypertension with ckd order carvedilol now. When confronted with the full-strength infectious virus arteria spinalis anterior purchase cheapest carvedilol and carvedilol, these primed cells react quickly and with greater intensity than unprimed cells hypertension of the eye buy cheapest carvedilol and carvedilol, thus enhancing the host�s ability to successfully combat and control the infection. Historically, three different routes have been taken in developing antiviral vaccines. This process, called atten uation, yields a form of the virus with just enough potency to cause an immune response but not enough to cause disease. The attenuated, live virus is then tested initially in animal models and later in human volun teers to assess its safety and immunizing capacity. This was the method followed to formulate the successful smallpox, measles, yellow fever, and Sabin poliomyelitis vaccines. By the second route, the virulent virus is Introduction to the Principles of Immunology 45 inactivated, essentially killed, by use of a chemical such as formalin. The killed virus is then tested for its capacity to cause an immune response as above. For the class I pathway, antigens inside cells from living, replicating viruses (virulent or attenuated) are broken into smaller components called peptides. Although this division is not absolute due to a process called cross-priming, it is an accurate generalization. The thymus is a two-lobed gland of the lymphoid system located over the heart and under the breastbone. They travel along the highways of blood vessels and wander among tissues throughout the body seeking cells that are foreign (not like self) because they express viral proteins or are transformed by cancers. They release soluble materials (proteins) that help or induce bone marrow� derived (non-thymic-educated) B lymphocytes to differentiate and make antibodies. Thus, T lymphocytes seek foreign antigens (in this case, viral antigens�peptides derived from the viral protein) on the surfaces of infected cells being parasitized by the virus. T cells that recognize an infected cell as �foreign� (contains virus) become activated and either directly kill the infected cell and/or release soluble factors (lymphokines, cytokines) that alert and arm other cells of the host to join the battle. In addition, some of these cytokines can directly interfere with viral replication. By such means, the spread of viruses is inhibited, and the nidus of infection removed. In fact, overall immunity has a built-in plasticity such that the relative contribu tion of each arm of the immune response varies according to the identity of an infecting virus. Antibodies primarily react with viruses in the body uids and are, therefore, most effective in limiting the spread of virus through the blood or in cerebrospinal uids that bathe the brain and spinal cord. By this means, antibodies decrease a host�s content of virus and diminish infectivity, thereby lowering the numbers of infected cells. As the number of virus particles released is reduced, the work of antibodies becomes easier. Before continuing the story of T lymphocytes (below), I�ll diverge here to describe antibodies, which are large protein molecules. Antibodies are made by B lymphocytes, named for their source, the bone marrow (1,2). B cells are small resting lymphocytes with nuclei that virtually ll these cells; little cytoplasm is present. When a virus or viral protein is encountered by a specic lymphocyte with a preconceived receptor for the antibody that matches the virus�s protein structure, the lymphocyte becomes stimulated to divide and the amount of cytoplasm composing the cell�s volume increases. The expanded cytoplasm factory then man ufactures antibodies designed to interact with the virus that stimulated their production and exports these antibody molecules into the immedi ate milieu. One such activated B lymphocyte can pump out 100 million antiviral antibody molecules per hour. Antibodies latch onto and neutralize viruses by one of several mech anisms: (1) Antibodies can coat or block the outer spike protein of the virus that attaches to receptors on a cell and initiates viral entry into the cell. Each anti body molecule generated acts on a specic antigen or target molecule of the virus. The host has the capacity to synthesize billions of different antibodies via genes that dictate their manufacture. Contraction of the target cell is accompanied by retraction of cell bers, thickening of the cytoplasm in the center of the cell, and nally by massive blebbing. Thereafter, the quantity of these cells contracts and is maintained at 1 to 2 percent of the total generated; these become immune memory cells (1,3�6). The number of antibodies then rises over a period of two to four weeks after infection, and they linger for years. B cells as well as T cells can be memory cells, that is, cells that were previously in contact with a particular virus. This is the likely scenario played out in those who survive infection from smallpox, measles, yellow fever, poliomyelitis, or hemorrhagic fever viruses. Lysis of the retrovirus produces holes (arrows), but lysis of the are navirus begins a progression of events that climaxes in the release of virus nucleic acids to the outside environment away from the protective virus coat. These genes encode proteins that protect the virus from harsh conditions during its transport from one host to the next; that is, they stabilize the infectious particle for travel through the environment. Also encoded are viral proteins that bind the virus to its receptors on cells, assist in internalization of the virus into cells, and provide the appropriate signaling for replication, assembly, and exit of the viral progeny from the parasitized cell. The second group of genes has among its main purposes the subjugation and/or modication of a host�s immune system. By such strategies the virus can manipulate the normal function of the immune system to escape surveillance and destruction for itself and the cells it infects. The story of this most universally feared disease, its elimination, and whether it could return again to cause havoc is the topic of this chapter. Two of the more interesting commentaries about this major accomplishment of mankind in eradicating smallpox from our planet is, rst, that considerable opposition stood in the way of its conquest 200 years ago, as well as in the recent past, and second, that signicant controversy remains about the possible return of smallpox and what to do about it. The plot to deliberately crash commercial airplanes into the twin towers of Manhattan�s World Trade Center announced to every country on the globe its vulnerability to fanatics who value death over life and have no regard for innocent civilians. This scenario of suicide bombings had played out earlier in the Middle East, Africa, Asia, and Europe. With the understanding that suicide attacks can kill large popula tions, the fear of deliberate biological attacks surfaced. Of the several devastating biological agents available, smallpox virus is at or near the top of the list. The seeds of those macabre investigations germinated in the hands of victorious Russian and American forces, as each developed their own biological warfare programs. Research into the offensive use of biologi cal weapons as agents of war was terminated unilaterally by the United States during the Nixon administration in the 1960s. Nevertheless, tests using indicator but relatively harmless bacteria continued to gauge dis persals of microorganisms over selected cities and in the New York City subway system. Thus, the technology was in place for dispersal but not for the intent to follow through. Yet, the Russian biowarfare program continued secretly during the Cold War and into the late 1980s based in part on the potential usefulness of biological reagents for terrorism or war and Soviet suspicions that the United States was secretly continu ing their biological warfare programs. However, with the September 11 attacks the sub-rosa testing programs changed into a very real possibility that smallpox could become a weapon in the hands of terrorist groups or rogue nations. When a biological agent becomes a candidate for weaponry, among the rst considerations is its virulence. Virulence refers to the ability of an organism, in this case the smallpox virus, to cause disease. Virulence factors are encoded within the genes of a virus and can be manipulated by present day technology to increase in potency beyond anything nature has yet provided. Before September 11, smallpox virus was known to come in two avors: smallpox major that was lethal to about one in three people so infected, and smallpox minor, a naturally occurring variant that killed as few as one of one hundred people infected. Smallpox is one of the largest viruses known, and the vast majority of its genes are similar between these major and minor forms. Thus, just a small number of genes that differ determines whether the number of deaths it causes is high rather than low. There is no doubt that smallpox virus major in its natural form or one altered to increase virulence would be the bioterror weapon of choice. Susceptibility refers to the predisposal of the host, in this case humans, to become infected.