

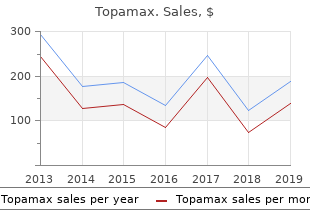
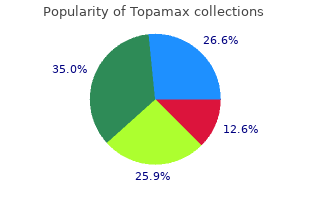
Topamax
"Order line topamax, medicine quiz."
By: Paul Reynolds, PharmD, BCPS
- Critical Care Pharmacy Specialist, University of Colorado Hospital
- Clinical Assistant Professor, Department of Clinical Pharmacy, Skaggs School of Pharmacy and Pharmaceutical Sciences, University of Colorado, Aurora, Colorado

http://www.ucdenver.edu/academics/colleges/pharmacy/Departments/ClinicalPharmacy/DOCPFaculty/Q-Z/Pages/Paul-Reynolds,-PharmD.aspx
Although the applica- French National Plan on Rare Diseases treatment kidney infection discount topamax online american express, and the German tion of strict criteria partly contradicts the concept of National Action League for People with Rare Diseases probabilistic reasoning symptoms before period generic topamax 100mg on-line, it is of great importance when [10 symptoms 3 months pregnant topamax 100 mg amex, 11 keratin smoothing treatment cheap topamax 100mg on-line, 35]. Integration of strict diag- a more efficient and targeted knowledge base extension nostic criteria separately from or after the probabilistic because it could enable integration of further related Ronicke et al. Orphanet Journal of Rare Diseases (2019) 14:69 Page 10 of 12 databases, such as existing databases of genetic variants. It would facil- Study limitations itate the integration of known disease genotypes, gene- A retrospective analysis of confirmed rare disease cases phenotype relations, as well as the appropriate suggestion is generally suitable to assess the potential accuracy of and handling of genetic tests in Ada. A strength of the study is that a wide of over 7000 known rare diseases and rapidly increasing range of diagnoses from the group of systemic inflamma- medical knowledge, the process of disease model creation tory diseases were represented (n = 42), including cases should be supported by technological means. However, results are limited to this group for future disease model creation should aim for curated, of diseases. Generalization of the results to the entire automated modeling from structured disease databases. Sim- tric design, a generalization of the study results applying ilar technology could be applied to keep the knowledge to other institutions or medical domains is limited. Although such a process should still be curated case input was not blinded to diagnosis, it was based by medical editors and follow rigorous quality testing, it on written documented information from the medical could accelerate the process of knowledge base extension records to reduce hindsight bias and retrospective misin- and maintenance. Future studies that aim to validate ther tests that are needed to confirm the correct diagnosis. For example, this can be achieved ment can be given regarding user dependency of the input. For this reason, this study, it can be speculated that improvement of such following studies should put an additional focus on user features might further facilitate early diagnosis. Orphanet Journal of Rare Diseases (2019) 14:69 Page 11 of 12 the optimization of the knowledge base during the course of multiple diagnoses, complex time-course information, of the study was accepted. Further knowledge base exten- To properly evaluate false positive suggestions, a suitable sion should be performed and existing databases should control group should be considered. Additional file Another limitation is that only confirmed conditions from the case set were added to the knowledge base Additional file 1: Data supplement. Arguably, contains summaries of the selected findings, attributes and factors for each case, including information from the diagnosis visit and from visits that a future extended disease knowledge base might lead lead to a correct top fit or top 5 fit suggestion. Early suggestion ranking of conditions could be lower if more diseases Acknowledgements were present in the knowledge base. The data are not publicly available due to them containing information that could compromise research participant privacy this study, but the results of early suggestion indicate and/or consent. Springer Nature remains neutral with regard to jurisdictional claims in Early diagnostic suggestions improve accuracy of family physicians: a published maps and institutional affiliations. Johns Hopkins University phenomena: Results of a German-wide expert Delphi survey. Hintergrundpapier - Defizitanalyse zur FindZebra - the search engine for difficult medical cases. Zurynski Y, Deverell M, Dalkeith T, Johnson S, Christodoulou J, Leonard H, 528–538. Clinical decision support systems for the practice of evidence-based Rare Dis (Austin, Tex). Available into the workflow of a teaching hospital service can decrease the cost of from:. S Scleritis sometimes occurs in an isolated fashion, without evidence of inflammation in other organs. However, in up to 50% of patients, scleritis is associated with an underlying systemic illness such as rheumatoid arthritis or granulomatosis with polyangiitis. Infection is an important but rare cause of scleritis, occurring in about 5–10% of all cases. Due to the similarity of its presentation, infectious scleritis is often initially managed as autoimmune, potentially worsening its outcome. Careful clinical history taking (including history of ocular surgery), detailed ocular examination, appropriate investigation for ocular disease with or without underlying systemic disease, and timely intervention has improved the long-term outcome for patients with this disease. Keywords Scleritis refers to a heterogeneous group of diseases characterized by inflammation of the sclera, Scleritis, infectious, autoimmune, vasculitides, which may also involve the cornea, adjacent episclera, and underlying uveal tract. This study of scleritis can be the initial manifestation of a potentially lethal systemic vasculitis or can be the involves a review of the literature and did not involve any 3 studies with human or animal subjects. Commons Attribution Noncommercial License, which permits any noncommercial use, distribution, adaptation, and reproduction provided the original author(s) and Specific etiologies of scleritis, varying from idiopathic to autoimmune to infectious, portend variable source are given appropriate credit. Scleritis sometimes occurs in an isolated fashion, without evidence Received: July 4, 2016 Accepted: August 26, 2016 of inflammation in other organs. However, owing to the similarity of its presentation, infectious scleritis is often initially managed as autoimmune, potentially worsening its outcome. Clinical features Scleritis can occur in any age group, but most commonly presents between the fourth and sixth decades of life; women are affected approximately twice as often as men. The redness has a bluish red appearance, tends to progress with time and can be sectorial or involve the whole eye. The pain is described as dull, aching, or boring and it may be severe and constant; it often awakens patients from sleep and is poorly responsive to analgesics. Patients complain of deep pain that radiates from the eye to the forehead, orbit and even the sinuses in some instances. Other complaints may include tearing, photophobia, and decreased vision (especially in posterior scleritis). The use of topical vasoconstrictors has minimal effect on these vessels and in contrast to episcleritis, the redness of scleritis will not be resolved with the instillation of 10% phenylephrine or 1:1000 epinephrine. These include keratitis, uveitis, glaucoma, exudative anterior scleritis retinal detachment, and macular edema. Anterior scleritis is much more frequent and can be further divided into diffuse, nodular, necrotizing and necrotizing without inflammation (scleromalacia perforans). Upon resolution the sclera may look bluish due to a rearrangement of the collagen fibrils, with no loss of tissue or thinning. Patients with nodular scleritis may progress to anterior necrotizing scleritis and this needs to be carefully monitored. This form of scleritis is also a sign of the onset of a potential lethal systemic vasculitis. The onset of necrotizing scleritis is gradual (3–4 days) and associated with Figure 3: Slit-lamp photograph depicting necrotizing severe pain. The affected avascular scleral tissue will look white and will be anterior scleritis surrounded by intense swelling and redness of actively inflamed tissue. The inflammation starts in a demarcated area and will spread circumferentially and involve the whole anterior segment. The damaged sclera will become translucent due to tissue loss and thinning, leaving the choroid covered by conjunctiva or residual thinned scleral tissue. The protrusion of choroid can occur with trauma or increased intraocular pressure. Systemic immunosuppression is required for the treatment of anterior necrotizing scleritis associated with autoimmune diseases. The damaged sclera is translucent due to tissue loss and thinning, leaving the choroid Scleromalacia perforans—This form of necrotizing scleritis without covered by conjunctiva and residual thinned scleral tissue. It is characterized by the painless and slow disappearance of the overlying Posterior scleritis episcleral tissue, associated with attenuation of the conjunctival and the onset of posterior scleritis has very few, and in some instances no physical episcleral vessels. The scleral tissue changes color from white to yellow signs, and the diagnosis can be challenging. Moreover, because posterior and this becomes absorbed and disintegrated, leading to exposure of the scleritis can present as a choroidal mass, serous retinal detachment, retinal underlying choroid. Although spontaneous perforation is rare, traumatic striae or retinal and disc edema, it is confused with other diseases of the perforations can easily occur. Routine testing typically Connective Tissue and Vasculitides Others Infections includes complete blood count, complete metabolic panel, urinalysis Inflammatory Diseases with microscopic analysis, perinuclear and cytoplasmic anti-neutrophil Rheumatoid arthritis Granulomatosis Rosacea Bacterial: cytoplasmic antibody, and chest X-ray. Mumps directed tests may include a tuberculin skin test, sacroiliac joint X-rays (for Ankylosing spondylitis Churg-Strauss Gout Fungal: spondyloarthropathy), sinus imaging (for Granulomatosis with polyangiitis), syndrome. Filamentous and viral hepatitis panel (hepatitis B for polyarteritis nodosa and hepatitis C. Psoriatic arthritis and Giant cell Chemical Inflammatory responses in the sclera can be granulomatous or non- Inflammatory bowel diseases arteritis injury granulomatous. Vessel occlusion and ischemia contribute to the evaluation of a patient with scleritis requires a systemic evaluation.
Always combined with Step 1 before or during sur- preferred treatment with strong consideration of gery patient preferences and circumstances the treatment 2014 order topamax now. Think of the stepladder more as a way to catego- usually be phased out within 6 months of rize patients based on severity medications similar to xanax order topamax 200mg with mastercard. Unilateral patients on Step 3 treatment may have of strategies to achieve the best outcome for the the inflammation in the fellow eye unmasked individual patient medicine vs nursing buy cheapest topamax and topamax. Area Review of Systems of inferior retinal neovascularization with vitreous ■ Reviewed 14 systems treatment viral conjunctivitis order cheapest topamax and topamax, negative except for above hemorrhage O. First described in the literature as chronic cyclitis ■ Masquerade syndromes by Fuchs in 1908 ● Primary intraocular lymphoma C. Standardization of Uveitis Nomenclature Working Group: Primary site of inflammation is the vitre- Workup ous. May be associated with systemic disease, such as multiple sclerosis or sarcoidosis. Intermediate uveitis accounts for 4%-8% of uveitis Treatment and Course seen in tertiary setting. Up to 25% of pediatric ■ After appropriate laboratory testing, a slow taper of oral referrals. Onset: Children and young adults psychiatrist) with concurrent initiation of corticosteroid- sparing immunomodulation. Bimodal distribution: second decade and third- reported recurrent suicidal ideation, aggression, and psy- fourth decade chosis. Blurred vision, floaters, photopsias, paracentral scoto- ■ Over the next few months, mycophenolate dose with mata increased to little effect. Antigenic basis of disease so far unknown ■ Pars plana vitrectomy with augmentation of peripheral laser and fluocinolone acetonide implant (Retisert) O. Retinal neovascularization with or without trac- tional membranes and vitreous hemorrhage 2. Primary site of inflammation is the vitreous (1-4+ globulin, toxoplasma IgG and IgM, Toxocara, Barton- vitreous cell/haze); can have mild anterior chamber ella: all negative or within normal limits inflammation B. Vitreal yellowish-white aggregates (snowballs); Final Diagnosis periphlebitis, exudates on the pars plana (snow- ■ Idiopathic intermediate uveitis / pars planitis bank): Do scleral depression C. Complications: macular edema, ocular hyperten- Clinical Course sion, retinal vascular leakage, cyclitic membrane formation, neovascularization, vasoproliferative ■ Topical steroids O. Idiopathic likely T-cell mediated ■ Plan to start systemic immunomodulatory therapy if he recurred C. Pars tion planitis: a 20-year study of incidence, clinical features, and out- comes. Special Considerations in the Pediatric Age Group Ophthalmology 2002; 109(1):95-98. Results of peripheral laser especially unilateral photocoagulation in pars planitis. Review of systems was completely nega- nephritis and uveitis syndrome in young patients with uveitis. Most patients present with either nonspecific symp- ■ Inflammatory bowel disease–associated uveitis toms such as fever, rash, flank pain / tenderness, ■ Psoriatic arthritis or fatigue, or they are completely asymptomatic ■ Syphilis except for ocular symptoms. Urine (not blood) beta 2 microglobulin is elevated Urinalysis and urine beta 2 microglobulin, basic metabolic as tubulointerstitial nephritis worsens. Proteinuria can be present, but albuminuria is do a biopsy based on clinical characteristics and overall absent as glomerular pathology is not common. Need to exclude other systemic diseases that can a urinalysis and urine beta 2 microglobulin (not blood). In cases with mild kidney dysfunction, oral steroids Discussion may be sufficient to control inflammation, but I. Introduction most patients will need long-term systemic immu- nosuppression to control the renal disease. Acute eosinophilic interstitial be caused by drugs or infections, but many cases nephritis and renal failure with bone marrow-lymph node granu- remain idiopathic. Prior to ● Tuberculosis referral to our center he had received a vitrectomy that had neg- ● Syphilis ative studies, including cytopathology. He was diagnosed with ● Endogenous endophthalmitis intermediate uveitis, which responded to oral and topical cor- ■ Noninfectious ticosteroids. Patient was started on antimetabolite therapy and ● Intermediate uveitis then advanced to infliximab due to lack of complete response ● Sarcoidosis of his uveitis. Despite advancement in therapy his intraocu- ● Undifferentiated anterior / intermediate uveitis lar inflammation eventuated to a robust amount of anterior chamber cell with plaque-like lesions in the anterior chamber of the right eye. There was 1+ anterior vitreous cell, no vitreous haze, ● Treponemal antibody: negative and no posterior segment lesions. Intermediate uveitis Anterior chamber paracentesis was negative by directed polymerase chain reaction and metagenomic deep sequencing B. Syphilis performed with biopsy of plaque-like material; this was positive for diffuse large B-cell lymphoma on cytopathology and immu- V. Intraocular lymphoma: update on diagno- latent Epstein-Barr virus has mediated the devel- sis and management. Spectral-domain opti- while most immunocompetent cases have not been cal coherence tomography and fundus autofluorescence findings related to an infectious pathogen. Classically, immunocompetent patients may develop disease in their fifth to sixth decades of 4. High-definition opti- cal coherence tomography features of primary vitreoretinal lym- life, while immunodeficient patients developed phoma. Vitritis, anterior chamber cell, or subretinal metagenomic deep sequencing identifies common and rare patho- involvement may be seen. Malignant: B cell lymphoma – may be localized only to the eye or involve the brain To explore how and when to evaluate the relationship of systemic disease and posterior uveitis using general C. Many diverse clinical presentations involving dots, History, clinical findings, and imaging drive the spots, plaques, etc. However, for a disease known to have no systemic associa- true understanding of the etiology may be lacking. Systemic Disease and Posterior Uveitis dromes do not present with simultaneous multisys- A. Always worthwhile to search for systemic disease tem findings; rather, they evolve over time. Causation, association, and unrelated coexistence associated tests that establish the diagnosis. Testing should be based on roiditis coexists in patients with posterior uveitis clinical findings and differential diagnosis. Viral serologies are rarely useful and are most use- ful when negative unless patient has systemic symp- B. To create collaborative interspecialty management nous choroiditis, hence serpiginous-like tubercu- to avoid duplication lous choroiditis. Mechanical: intraocular foreign body / ocular isch- ance or response justifies more testing. Review on and progression, then make an initial hypothesis the worldwide epidemiology of uveitis. Past medical history is notable for borderline diabetes, treated with diet and exercise modification. Slit lamp examination of the left eye is notable for 1+ pigmented cell in the anterior vitreous. Fundus examination reveals prominent midperipheral, perivenous sheathing and exudates. There are scattered, diffuse intraretinal hemorrhages, as well as old vitreous hemorrhage adjacent to the inferotem- poral arcade. Wide-field angiography demonstrates segmental leakage along the retinal veins, with marked nonperfusion in the superior and temporal midperiphery and periphery. Periphlebitis often segmental Sarcoidosis, Behçet disease, pars planitis, antineutrophil cyto- 3. Chest x-ray may demonstrate hilar adenopa- erythematosus, tuberculosis, multiple sclerosis, syphilis, Lyme thy or pulmonary infiltrates. Corticosteroids (topical / oral / periocular / intravitreal) are a mainstay of therapy.
Positive response to ice water test associated with high-grade bladder outlet obstruction in patients with benign prostatic hyperplasia symptoms of anxiety generic 100 mg topamax with visa. Comparison of parameters to determine the cause of urinary disturbance in men with prostate volume less than 20 milliliters treatment nurse purchase 100mg topamax. A case of a large inguinoscrotal bladder hernia secondary to benign prostatic obstruction medicine 7767 buy generic topamax 100 mg online. A prospective study of the efficacy of Serenoa repens treatment of shingles cheapest topamax, tamsulosin, and Serenoa repens plus tamsulosin treatment for patients with benign prostate hyperplasia. Clinical observations of the effect of antidiuretic hormone on nocturia in elderly men. Characterization of human chorionic gonadotropin in normal and abnormal pregnancies. Relationship of prostate-specific antigen and prostate volume in patients with biopsy proven benign prostatic hyperplasia. Decreased suburethral prostatic microvessel density in finasteride treated prostates: a possible mechanism for reduced bleeding in benign prostatic hyperplasia. Lasers for lower urinary tract symptoms secondary to benign prostatic hyperplasia: when is the fuss worth it. Evaluation of the cytokines interleukin 8 and epithelial neutrophil activating peptide 78 as indicators of inflammation in prostatic secretions. Holmium laser enucleation of the prostate combined with electrocautery resection: the mushroom technique. Value of free prostate-specific antigen (Hybritech Tandem-R) in symptomatic patients consulting the urologist. Misclassifying the indications for prostate-specific antigen testing may bias case-control studies of the efficacy of prostate cancer screening. Transurethral microwave thermotherapy vs transurethral resection for treating benign prostatic hyperplasia: a systematic review. Laser prostatectomy versus transurethral resection for treating benign prostatic obstruction: a systematic review. Intraprostatic temperature monitoring during transurethral microwave thermotherapy: status and future developments. Quantification of prostate shrinkage after microwave thermotherapy: a comparison of calculated cell-kill versus 3D transrectal ultrasound planimetry. Safety and efficacy of tolterodine extended release in men with overactive bladder symptoms and presumed non-obstructive benign prostatic hyperplasia. Chronic sacral neuromodulation for treatment of neurogenic bladder dysfunction: long-term results with unilateral implants. Crystallization during volume reduction of solutions with a composition corresponding to that in the collecting duct: the influence of hydroxyapatite seed crystals and urinary macromolecules. Racial differences in pathogenetic mechanisms, prevalence, and progression of benign prostatic hyperplasia. The detrusor muscle cell in bladder outlet obstruction-ultrastructural and morphometric findings. Mortality and prostate cancer risk in 19,598 men after surgery for benign prostatic hyperplasia. Infectious disease hospitalizations among older American Indian and Alaska Native adults. Is bladder dysfunction and incontinence associated with ureteroceles congenital or acquired. Classification of nocturia in the adult and elderly patient: a review of clinical criteria and selected literature. Pressure-flow studies in benign prostatic hyperplasia: to do or not to do for the patient. Nocturia in the adult: classification on the basis of largest voided volume and nocturnal urine production. Significance of nocturia in the International Prostate Symptom Score for benign prostatic hyperplasia. Symptom assessment tool for overactive bladder syndrome-overactive bladder symptom score. Comparative study of concentration of isoflavones and lignans in plasma and prostatic tissues of normal control and benign prostatic hyperplasia. Identification of baseline clinical factors which predict medical treatment failure of benign prostatic hyperplasia: an observational cohort study. The importance of patient perception in the clinical assessment of benign prostatic hyperplasia and its management. Cadmium-induced acute hepatic injury is exacerbated in human interleukin-8 transgenic mice. The short-term effects of tamsulosin in Japanese men with benign prostatic hyperplasia. The short-term effects of terazosin in Japanese men with benign prostatic hyperplasia. The problem of cutoff levels in a screened population: appropriateness of informing screenees about their risk of having prostate carcinoma. Predictive value of total and percent free prostate specific antigen in high grade prostatic intraepithelial neoplasia lesions: results of the Tyrol Prostate Specific Antigen Screening Project. Lower levels of nuclear beta-catenin predict for a poorer prognosis in localized prostate cancer. Brachytherapy for prostate cancer: follow-up and management of treatment failures. Pre-clinical evidence for the use of phosphodiesterase-5 inhibitors for treating benign prostatic hyperplasia and lower urinary tract symptoms. Cell death mechanisms associated with G2 radiosensitivity in patients with prostate cancer and benign prostatic hyperplasia. Impact of interventional therapy for benign prostatic hyperplasia on quality of life and sexual function. Ultrastructural and biophysical studies on protein conformations of epithelium and stroma in benign prostatic hyperplasia before and after transurethral resection of the prostate. Reduced 1alpha-hydroxylase activity in human prostate cancer cells correlates with decreased susceptibility to 25-hydroxyvitamin D3-induced growth inhibition. Cloning of two novel mammalian paralogs of relaxin/insulin family proteins and their expression in testis and kidney. Deficient nucleotide excision repair capacity enhances human prostate cancer risk. Immunohistochemical analysis of Omi/HtrA2 expression in prostate cancer and benign prostatic hyperplasia. Applicability and reproducibility of condom catheter method for measuring isovolumetric bladder pressure. Association of vitamin D receptor FokI polymorphism with prostate cancer risk, clinicopathological features and recurrence of prostate specific antigen after radical prostatectomy. Chronic kidney disease after nephrectomy in patients with renal cortical tumours: a retrospective cohort study. Correlation between voiding and erectile function in patients with symptomatic benign prostatic hyperplasia. Haplotypes, loss of heterozygosity, and expression levels of glycine N-methyltransferase in prostate cancer. Initial experience with successful totally robotic laparoscopic cystoprostatectomy and ileal conduit construction in tetraplegic patients: report of two cases. Epithelial cell differentiation pathways in the human prostate: identification of intermediate phenotypes by keratin expression. Community study of uncomplicated lower urinary tract symptoms among male Italien immigrants in Sydney, Australia. Glomerular volume and clinicopathologic features related to disease severity in renal biopsies of African Americans and whites in the southeastern United States. Evaluation of microwave thermotherapy with histopathology, magnetic resonance imaging and temperature mapping.
Purchase topamax 200mg without a prescription. Withdrawal symptoms after 5 days without Marijuana.