

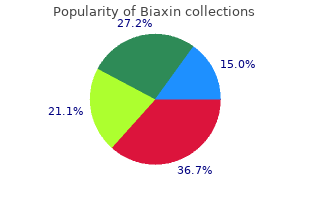
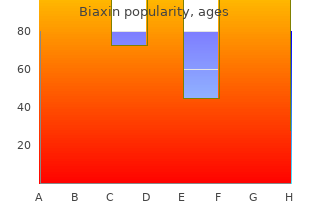
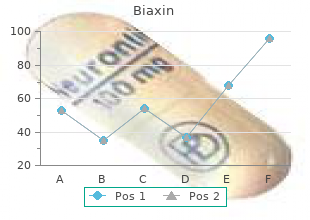
Biaxin
"Biaxin 250mg without a prescription, gastritis black stool."
By: Paul Reynolds, PharmD, BCPS
- Critical Care Pharmacy Specialist, University of Colorado Hospital
- Clinical Assistant Professor, Department of Clinical Pharmacy, Skaggs School of Pharmacy and Pharmaceutical Sciences, University of Colorado, Aurora, Colorado

http://www.ucdenver.edu/academics/colleges/pharmacy/Departments/ClinicalPharmacy/DOCPFaculty/Q-Z/Pages/Paul-Reynolds,-PharmD.aspx
One research group has studied 1 gastritis diet 2015 biaxin 500 mg on-line,200 people between with Huntingtons disease (which causes memory loss gastritis diet 800 cheap 250mg biaxin fast delivery, the ages of seventy and eighty gastritis diet ���� purchase 500 mg biaxin fast delivery. Would knowing your people for ten years bile gastritis diet cheap 500mg biaxin amex, the researchers found that the ones fate make you live your life differently, or would you just start who kept their excellent mental functioning had three traits carrying the burden of the disease that much earlier Nowadays, however, America glorifies youth, and all too often the elderly are seen 2. At present there is no definitive laboratory test for as comical, querulous and infirm. As the countrys popula Alzheimers disease and no cure, though some medications tion ages, what steps could we take as a society to give can help ameliorate the symptoms. Raise the retirement identified many of the genes that confer an increased risk for age, for example Have mediation sessions in nursing the disease, its possible that a genetic test will become homes, where minor grievances are aired before a panel of available. Brush your teeth with the opposite hand, take the side Try gardening, playing chess or even memoir writing. It may sound off-the-wall, Defer retirement, mentor others in your field, take up but creating new associations � even arbitrary ones � challenging causes, travel to exotic lands, step up your is tantamount to brain-building. Ask the bus driver his name, Memory is not just for sights and sounds, but for tex start a conversation, recall his name on the next occa ture, emotions and even smell. If he tells you his son is taking tuba lessons, make Asian market and get to know the spices and unfamiliar a note to ask him how the boy is progressing. Find hobbies, take classes or do work that uses also about creating new, more dynamic ones. Reading, from short stories to Tolstoy, is a For more information on improving your memory, visit: great brain-builder, as are classes in anything from. It occupies ticity underlies everything the brain the normal programs of neuronal a certain amount of space: 8 1/2 inch does. But this normal wear experience new connections and tear doesnt bring are formed. Change the expe about any basic modifica rience, and you change the tion to the size of the brain. Abnormalities will lar terms � that once it also occur if, because of pre reached a certain level of mature birth, the brain enters development it remained the world too soon and is pretty much the same overwhelmed with more except for some biologi stimuli than it is equipped to cal wear and tear (loss of handle. At the conclusion the brain remains a of infancy, a sculpting dynamic structure that process begins, becoming the alters from year-to-year, dominant force shaping the day-to-day, even moment brain. Thanks Next come the formation of the major contains many more neurons than it to what neuroscientists call plasticity, brain regions and a migration of neu requires, so excess neurons are pruned the brain possesses amazing capacities rons from their original sites of gener away according to the most funda for change. Indeed, most congenital (present that are used are strengthened and (continued) B Essay 1 The ing ones career results in the forma tips of the fingers undergoes measura neurons established during gestation tion of new networks composed of ble changes in blind readers of Braille and infancy are thinned out in millions of nerve cells. Thanks to this process limits his or her experiences, or fails new challenges and opportunities. Most interesting is the finding pally as a holding operation, an dren vastly increase their abilities to that important brain changes can attempt to retain past gains while pay attention and remember and occur in extremely short periods of yielding as little as possible to decline begin mastering the universe. We now know that such a brain that receives impulses from the view is unduly pessimistic. Thus the older person Essentially, stem cells are primitive the likely consequences of ones has a choice: Accept the stereo unspecialized cells that can �morph� into mature actions, planning, reasoning and types about aging and sit in a cells while continuing to multiply and provide a controlling ones emotions. Since their frontal lobes are not Stem cells in the skin and bone account for the fully developed, adolescents While the aging brain may be a healing that took place. Stem cells also give birth sometimes exhibit such frontal bit slower in learning, manipu to the cells in the liver, the lining of the intestines, lobe-based difficulties as impul lating and rapidly retrieving and all the cellular constituents of the blood. The siveness, foreshortened attention discovery of stem cells within the brain suggests new information (one of the spans, and failure to realize the they are capable of turning into adult neurons. Once the growth the brain, end up in specific locations and then adults), it remains highly plas and pruning process has been suc fully differentiate into neurons,� explains Fred tic and adaptable. For cessfully completed, adolescents Gage, Professor of Genetics at the Salk Institute. And thats younger colleagues when it continues but without the dra really a key feature in understanding the larger comes to integrating new matic level of pruning observed picture of what plasticity is all about. But one doesnt the adult, plasticity involves the place for the treatment of dementia: the induction have to be a college professor formation and maintenance of of nerve cell multiplication and the replacement to possess these talents. Both of these strate his essay �On Old Age,� gies could potentially treat presently incurable on ones interests and activities. Nurture and the Individual Child by Sandra Ackerman �She gets that easygoing temperament According to psychologist Eleanor �The concept of nature versus nurture from her father,� a mother may say, as Maccoby, we are neither and we are is so ingrained in our thinking,� says her two-year-old sits happily dumping both. Or, tions and their parents childrearing ology, psychology and pediatrics at applauding an eight-year-old after his regimes,� Dr. Maccoby says, express the University of Alabama, �its first school concert, the parents may ing the predominant view of develop almost impossible to get beyond. Perhaps because chil that determines how a child dren keep surprising us will think, feel and behave. From generation to genera tion, the more curious Although all siblings emerge among us have wondered from the same gene pool, each how we can each start out one receives a unique set of as a single fertilized cell genes: some from the mother and yet become a unique �I� with our closely interwoven. They function and others from the father, some dom own thoughts, feelings and behavior. Then, even in the most stable family, this new popularity arose from a single scientific paper pub each childs experience will be differ lished in 1993, in which a research team showed that listening to ent. The parents may be new at rais Mozarts music improved the performance at certain mental tasks of ing children or old hands at it; the sib elementary school students. Gradually, as the story was reported to lings are older, younger, all of one sex larger and less specialized audiences, this finding grew in perceived importance, until the so-called �Mozart effect� was said to increase or the other, or mixed; household cir babies overall ability to learn or even in some way to enhance their cumstances may be comfortable or brain for life. At the same time, though, further scientific studies did difficult; the family may exist in a not confirm these results, and soon the exaggerated claims for the long-established network of friends Mozart effect began to appear to be just that. All nal study: not only did the students improved performance on the test these factors together form the fail to carry over to other kinds of schoolwork, but it also proved to be childs microenvironment, rather short-lived. The furor over the Mozart effect has largely died and they produce major down, but the story of its popular rise and fall lingers as a warning and lasting effects. Genes can set up a tenden cy or predisposition toward certain likes or dislikes, talents, levels of energy, and even self image. But these ten dencies may fit well or How the child responds to such a label, and badly into the childs what she has made of her own inherited environment � above traits and experiences so far, will have an all his home environ impact on the way her family perceives and ment � in ways that fur treats her, which may in turn modify her ther shape the childs traits self-image and her dealings with parents and view of himself. In a and siblings, and so on, in a cycle lasting family fond of sports and well into adulthood. Paradoxical as it games, for example, a less seems, each child takes part in creating actively inclined child may the very environment that helps to shape be encouraged to join in, or her as a unique person. We able to watch the equivalent of an Scientists learned this from early know this because addictive drugs incredibly scintillating game of pin experiments with rats. When lab rats mimic the action of one or more of the ball, as the pleasure centers light up eat or become sexually aroused, brains neurotransmitters. And as a and play off one another in response dopamine levels increase in the areas result of this successful mimicry, the to the steak. But the same thing brain is fooled into responding as it happens when rats inject themselves would to the natural neurotransmitter. If you dont fancy steak, think about with addictive drugs like cocaine, for �The drugs do that,� says Steven whatever else �turns you on� � a example, by pressing a lever or turning Hyman, director of the National term, incidentally, that provides an a wheel. They will repeat these behav Institute of Mental Health, �by tap apt description of what is happening iors hundreds of times to experience ping into the brain-reward sys the pleasure set off by the tem and fooling that system. The brain-reward system is Liz, a patient at the Caron made up of areas of the brain foundation in Wernersville, collectively referred to as the Pennsylvania, which specializes pleasure centers. Most impor in the treatment of cocaine and tant is a pathway that starts in other substances of abuse, the brainstem and extends described a similar craving. Increasing the level of dopamine in these Lizs experience illustrates the areas increases their neuronal key feature of addiction, firing rate; decreasing the according to George Koob, dopamine level decreases the professor of pharmacology at firing rate. Your pleasure centers have mignon (assuming youre not a vege skiing, travel or parties, the brains been usurped, taken over by the tarian). You no longer seek natural of steak, neural messages fire within �turning on,� of those pleasure cen pleasures because the drug is driving this dopamine pathway.
These data suggest that the cardiac teratogenicity of lithium has previously been overestimated gastritis bacteria cheap 250 mg biaxin amex. Of the two studies versus lithium gastritis diet ������ buy biaxin 250 mg fast delivery, one found a superiority of this drug over carbamazepine (response rate: 79% versus 29%) which gastritis menu biaxin 250mg sale, however gastritis juicing recipes biaxin 250 mg with amex, 360 M. Bartoli did not reach statistical significance, and the other reported no difference between the two drugs. Both studies versus chlorpromazine found no difference between this neuroleptic and carbamazepine. A double-blind study has shown that a lithium-carbamazepine combina tion is as effective as the association of lithium and haloperidol in the treatment of a manic episode (Small et al. The former less frequently produces extrapyramidal effects, but more often requires the addition of a benzodiazepine during the first week. According to currently available knowledge, carbamazepine should be regarded as a valid alternative to lithium in the treatment of manic episodes. There is no convinc ing evidence of a superiority of carbamazepine over lithium in the treatment of mixed mania. The evidence of an efficacy of carbamazepine in depressive episodes of bipolar disorder is much weaker. Some other very small con trolled trials and several open studies do not add significantly to the above evidence. Prevention of recurrences of bipolar disorder At present there is only one double-blind placebo-controlled trial of car bamazepine in the prevention of recurrences of bipolar disorder (Okuma et al. Of these studies, three found carbamazepine to be as effective as lithium, while one (Watkins et al. However, the difference in favour of lithium became significant when, in addition to recurrences, the need for neuroleptics and / or antidepressants for at least 6 months was considered as failure. It has been maintained that bipolar patients who respond to carbamaze pine prophylaxis, compared with those responding to lithium, less often have a positive family history of bipolar disorder and are more frequently rapid cyclers (Kishimoto et al. However, a retrospective study con ducted in 215 bipolar patients treated with lithium or carbamazepine for 2 years (Okuma 1993) found that rapid cycling predicts a poor response to both drugs. It has been reported that at least half of patients who respond initially to carbamazepine have a recurrence after 3�4 years (Post et al. The combination of lithium and carbamazepine may be useful in some bipolar patients who do not respond satisfactorily to either drug. The combination of lithium and carbamazepine is usually safe, although one case of neurotoxicity has been reported. Via the cytochrome P450 3A3 / 4 system, carbamazepine induces its own metabolism (so that its half-life may decrease during long-term treatment from 18�55 to 5�26 hours, requiring dosage adjustment) and that of several other drugs, including valproate, haloperidol, clozapine, imipramine and oral contraceptives, whose plasma levels are therefore reduced. Several drugs inhibiting the above cytochrome may slow carbamazepine metabo lism, increasing its plasma levels: they include valproate, selective serotonin reuptake inhibitors and some antibiotics. Side-effects the most common side-effects of carbamazepine are neurological: fatigue, blurred vision, nausea, dizziness, headache, motor incoordination, diplopy, nystagmus. Bartoli A transient leukopenia has been found in about 10% of patients treated with carbamazepine. It does not predispose to infections and usually resolves spontaneously or after dose reduction. In about five cases out of 1 million, carbamazepine may cause aplastic anaemia and in about 1. These reactions are potentially fatal and are not predictable by monitoring drug plasma levels or by the occurrence of the above-mentioned mild haematological side-effects. In most cases these severe adverse reactions occur in the first 3�6 months of treatment. It can manifest itself with symptoms (nausea, headache, dizziness) and require treatment discontinuation. An asymptomatic increase of liver enzymes has been found in 5�10% of patients treated with carbamazepine. It has no relationship with the rare, idiosyncratic and unpredictable hepatic failure, usually occurring during the first month of treatment, which may be fatal. In most cases they are mild and not accompanied by other symptoms, and resolve spontaneously. In rare cases a skin rash may be part of a widespread reaction caused by hypersensitivity to the drug, including fever, hepatosplenomegaly and lymphadenopathy, with a pos sible involvement of other organs (myocarditis, interstitial pneumonia, pseudolymphoma, interstitial nephritis). In very rare cases carbamazepine may cause serious and potentially fatal skin reactions such as exfoliative dermatitis, Stevens�Johnson syndrome, and Lyell syndrome. Carbamazepine has been involved in rare cases of pancreatitis, heart failure, hypertension, cardiac conduction disturbances and renal failure, and in sporadic cases of psychosis. The use of carbamazepine during the first trimester of pregnancy has been associated with an increased risk of neural tube defects and craniofacial malformations. The frequency of neural tube defects can be reduced by prophylactic treatment with high doses of folate. Mood stabilizers in bipolar disorder 363 the drug has been found to be significantly superior to placebo, and as effective as lithium. Pooling the results of the three studies, 54% of patients treated with valproate showed a reduction of at least 50% of manic symp tomatology. Contrary to lithium, valproate was equally effective in mixed and classic mania (Swann et al. In a randomized trial of valproate oral loading (20 mg / kg per day) versus haloperidol (0. The greatest rate of improvement for both treatments occurred during the first three full days of administration (McElroy et al. According to currently predominant consensus (Expert Consensus Panel 1996, Suppes et al. There is no controlled trial of valproate in the treatment of depressive episodes of bipolar disorder, and open trials have reported response rates consistent with a placebo mechanism of action (American Psychiatric Association 1994). Prevention of recurrences of bipolar disorder No controlled trial of valproate in the prevention of recurrences of bipolar disorder has been published as yet, but the preliminary results of a 1-year double-blind placebo-controlled trial (Bowden 1997) suggest a significant superiority of the drug over placebo in increasing the time in remission, and several open trials indicate that the drug may reduce the frequency and severity of affective episodes, also in rapid cyclers (McElroy et al. In a randomized trial in which 12 bipolar patients received either valproate or placebo in association with lithium, those treated with lithium and valproate were significantly less likely to suffer a recurrence (Solomon et al. The valproate dose range recommended for the prophylactic purpose is 750�2000 mg/day. Side-effects Common, dose-related side-effects of valproate are gastrointestinal distur bances (nausea, vomiting, anorexia, dyspepsia), observed in up to 25% of treated patients; a transient asymptomatic increase of hepatic transaminases; tremor, drowsiness; trombocytopenia, leukopenia and inhibition of blood 364 M. Rare, idiosyncratic and potentially fatal adverse reactions are irreversible hepatic failure, acute haemorrhagic pancreatitis, and agranulocytosis. The exposure to valproate during the first trimester of pregnancy has been associated with an increased risk of neural tube defects. Of the 41 patients who were currently depressed, 18% displayed moderate and 53% marked improvement. Of the 31 patients who were currently in a manic, hypomanic or mixed episode, 3% showed moderate and 81% marked improvement. Improvement was significant among both rapid cyclers and non-rapid cyclers; however, while in patients who were currently depressed the improvement in depressive symptom atology was equivalent in the two groups, in those who were in a manic, hypomanic or mixed episode the improvement in manic symptomatology was more pronounced in non-rapid cyclers (Bowden et al. Dizziness, headache and skin rashes were the most frequent side-effects, and led to treatment discontinuation in 10 patients (13%). According to the preliminary results of an ongoing double-blind placebo controlled trial (Frye et al. Concomitant treatment with valproate increases the blood levels of lamot rigine, which may cause an increased frequency and severity of skin rashes (Peck 1991). Gabapentin the largest available open trial of gabapentin in bipolar disorder (Shaffer and Shaffer 1997) used the drug as add-on or in monotherapy in 28 bipolar patients refractory to treatment with lithium, valproate or carbamazepine. A "positive response as judged by both the treating psychiatrist and the patient" was observed in 18 cases. Eight patients interrupted treatment Mood stabilizers in bipolar disorder 365 because of intolerable side-effects (of which the most common were oversedation and overactivation) and two due to inadequate response. The combination of gabapentin with lithium, valproate or carbamazepine appears to be safe. An update on the biological effects of lithium and anticonvulsants which may be relevant to their clinical activity can be found in Manji et al.
However gastritis diet ������ cheap biaxin 250 mg free shipping, graded activity programs using a behavioral approach seem more effective than traditional care for returning patients to work and reducing sick-leave gastritis raw food diet buy discount biaxin on-line. The original systematic reviews on which these guidelines are based on are the 103 gastritis diet ��������� buy discount biaxin 500mg line, 174 gastritis severe pain purchase 250 mg biaxin with visa, 175 reviews by van Tulder et al. The main original studies cited are the studies by 173 176 177 178 179 Turner et al. Cognitive-behavioral interventions versus placebo All guidelines agree to conclude that cognitive-behavioral interventions are more effective than placebo or no intervention (waiting list controls). This Cochrane concluded that evidence is strong that behavioral treatment (combine respondent-cognitive therapy) is superior to waiting list control (based on four studies; 134 patients) and alleviates pain moderately. It also concluded that there is moderate-quality evidence that progressive relaxation has a short-term positive effect on pain and behavioral outcomes (based on 2 trials; 39 patients). On the other hand, operant treatment is no more effective at short-term than waiting list control (strong evidence; based on 2 trials; 87 patients) in terms of general functional status and on behavioral outcomes (moderate-quality evidence; based on 3 trials; 153 patients). It concludes that there is no evidence available supporting the superiority of any cognitive-behavioral method. More intensive programs seem more effective than less intensive ones, especially in terms of return to work and improvement of physical capacity. There is conflicting evidence on the safety of spinal manipulations in low back pain. There is no difference in terms of effectiveness between the different types of behavioral interventions. The patient takes these medications either continuously or for shorter periods of time during recurrent episodes of pain. This reference does not specifically focus on neuropathic pain of 186, 187 lumbar origin. In this study, tramadol/paracetamol association was found to significantly improve pain, disability (Roland Morris) and quality of life. Safety of weak opioids 187 the systematic review by Schnitzer reports that safety results vary between studies. Patients withdrawals due to adverse effects varied from 4% to 35% according to the studies. The potential adverse effects of such medications are important, including physical addiction. The most frequent adverse effects are constipation, urinary retention, liver pain and effects on central nervous system. Finally, side effects at long-term have been understudied although they are known to be frequent and harmful. These conclusions are supported by the systematic reviews of 160, 184 van Tulder et al. Rofecoxib has been withdrawn since then given its higher risk for cardiovascular effects. Studies were medium or low quality, with small sample size and lack of placebo-control design. Cox 2 inhibitors have been shown to have a better gastro-intestinal safety profile in osteoarthritis and rheumatoid arthritis studies. However, one of these drugs (rofecoxib) increases cardiovascular risk (myocardial infarction and stroke) with long 202 term use (> 18 months). Adverse effects of muscle relaxants drugs should be kept in mind as they are far from being negligible. Non-benzodiazepine muscle relaxants There is conflicting evidence that non-benzodiazepines alleviate pain and that they 2 reduce muscle spasm. However, the two high-quality trials mentioned above showed that neither flupirtin nor tolperisone were associated with a higher 207, 206 incidence of adverse events compared with placebo. It is known that tolperisone can have severe allergic side effects and that flupirtin can induce reversible reduction of liver function. For gastrointestinal events, the common complaint is nausea but the 208 difference between muscle relaxants and placebo seems not significant. Recent guidelines and systematic reviews conclude that noradrenergic and noradrenergic-serotoninergic antidepressants are moderately effective. There is moderate-quality evidence that activities of daily living (function, disability) are not improved by antidepressants (level B). In five of them antidepressants were more effective than placebo in reducing pain and depression. Safety of antidepressants 187 the review of Schnitzer et al estimated that withdrawals due to adverse effects ranged from 20% for fluoxetine (6-weeks long study) to 44% for amitriptyline/atropine (16-weeks long study). In many trials, the reporting of side effects was insufficient, so this percentage probably underestimates the degree to which they occurred. Patients with renal disease, glaucoma, pregnancy, chronic obstructive pulmonary disease and cardiac failure should not be treated with antidepressants. It must however be noted that, in that study, patients with neuropathic radicular pain were excluded. There was no difference in pain relief between the doloteffin group and the rofecoxib 3 214 group. The recent Cochrane systematic review concludes that Harpagophytum procumbens (50 to 100 mg/day), Salix alba (White willow bark: 120 to 240mg/day) and capsicum frutescens (topical) seem to reduce pain more than placebo. These conclusions are based on two references: one 216 217 systematic review by Mason et al. Moreover, the secondary effects of such drugs are known to be relatively frequent and harmful. Noradrenergic and noradrenergic-serotoninergic antidepressants seem moderately effective. These invasive procedures encompass a wide variety of techniques, such as injections, acupuncture, radiofrequency denervation, adhesiolysis, surgery and spinal cord stimulation for failed back surgery syndrome. Most of them are minor and transient but also rare major adverse effects and complications of such procedures have been described in case reports and non-randomized trials. These publications seldom register side effects in a uniform way and they do not allow determining neither precise incidences nor the clinical importance. Hence, the comments on possible adverse effects and complications that are available in the selected references are included in the safety sections of this report, when relevant. Those safety sections should not be considered as an exhaustive list of all possible adverse effects and complications. They are just mentioned as complementary information but the precise incidences can not be determined for each procedure. An additional search for 219 systematic reviews identified two Cochrane reviews: the review by Nelemans on 220 injection therapy and the review by Yelland on prolotherapy. This invasive technique 2 commonly used aims at alleviating radicular pain of lumbosacral origin. Various glucocorticoids can be used, alone or in combination with a local anesthetic or saline. Evidence of low-quality can be found for the effectiveness of transforaminal epidural steroid injections for sciatica (except in extruded disc herniations). However, the study populations were mixed groups of patients suffering chronic and sub-acute low back pain with sciatica. Major side effects or complications seem very uncommon but can potentially be dramatic. Among them, the fact that injections are performed without any X-ray guidance in many studies may be a concern, as it is well known that many unguided injections do not 2 reach their target. Unfortunately, since our search, the review has been withdrawn from the Cochrane site in relation with an updating process (searching period of this review being 10 years old). In this study, epidural steroids were administered blindly (with no X-ray guidance) in patients presenting sciatica (� 33% of patients with acute sciatica and 66% of sciatica of more than 1 month duration). This pragmatic study shows that benefit, in terms of a 75% improvement of Oswestry scores, was present but transient as only observed at the 3-weeks follow-up. No benefit was demonstrated from 6 to 52 weeks and no benefit was demonstrated for repeated epidural injections over single injection. It must be pointed out that the inclusion criteria for sciatica in this paper do not correspond with the criteria for chronic low back pain as defined in this report. The first study comparing transforaminal epidural steroid with local anesthetic shows a short effect for the steroid group but a rebound effect at 231 3 and 6 months, where the control group performed better.
Syndromes
- Gallbladder disease
- CT scan
- Nerves in the body can become damaged, causing pain, tingling, and a loss of feeling, problems digesting food, erectile dysfunction
- Foamy appearance of urine (due to large amounts of protein)
- The mother has type 1 diabetes, lupus, or phenylketonuria
- Rapid heart rate
- Migraine headaches
The investigators found that divalproex oral loading and haloperidol were equally effective in improving manic symptoms gastritis fish oil purchase biaxin 250 mg line. The findings of this study suggested that divalproex sodium was as effective as haloperidol diet during gastritis attack 500 mg biaxin with visa, not only in terms of reductions in manic symptoms gastritis ibs diet buy biaxin 250 mg without prescription, but also of psychotic symptoms; with both drugs showing significant improvement after 3 days of treatment gastritis symptoms upper right quadrant pain cheap biaxin on line. The investigators concluded that divalproex sodium was as effective as haloperidol, but offered a more benign adverse effect profile. The investigators found that, by week one, 32% of patients randomized to haloperidol and 23% randomized to chlorpromazine showed significant improvement. Tohen penthixol and haloperidol found that the two drugs were equally effective in overall efficacy and action in acute mania (Baastrup et al. Primozide One of the most potent typical antipsychotic drugs, primozide, has also been studied in the treatment of acute mania. The investigators found an initially faster response with the use of chlorpromazine, as mea sured by the Beigel�Murphy Mania Rating Scale. The authors concluded that the initial effects of chlorpromazine appeared to be related to sedative effects. In summary, typical antipsychotic agents have been used in the treatment of mania since they first appeared in the early 1950s. High-potency typical antipsychotics such as haloperidol or primozide appear to be more effective and have a faster onset of action than chlorpromazine. A major concern that remains regarding the use of typical antipsychotics is their adverse effect profile, including tardive dyskinesia, hyperprolactinaemia, and neuro leptic malignant syndrome. In addition, typical antipsychotics have been found to be depressogenic (Kukopulos et al. Considering their possible depressogenic effects, the use of typical anti psychotics in acute mania appears limited as they have only a unidirectional therapeutic effect. The latter is defined as an improvement of the symptoms of acute mania, but lack of improvement in the symptoms of depression or even worsening of depressive symptoms. This limitation has restricted the use of typical antipsychotic agents to the acute phase of the condition. It has been estimated that more than 85% of patients with acute mania receive a typical antipsychotic agent (Tohen et al. With the availability of the newer antipsychotic agents that provide a more benign adverse effect profile, and possibly mood-stabilizing proper Antipsychotics in acute mania 377 ties, there has been renewed interest in the use of antipsychotic agents in the treatment of acute mania. Some investigators have suggested that bipolar patients may have an increased risk of developing acute dystonia, akathisia, and tardive dyskine sia (Nasrallah et al. An additional risk associated with the typical antipsychotic agents is neuroleptic malignant syndrome. A possible association between affective disorders and tardive dyskinesia has been reviewed by a number of investigators. Kane and Smith (1982) found that the cumulative risk of developing tardive dyskinesia after being exposed to neuroleptics for at least 6 years was 26% for bipolar patients, compared to 18% for patients with schizophrenia. On the other hand, other investigators have not found a higher risk treating affective disorder patients. Specifically, Morgenstern and Glazer (1993), in a 5-year, follow-up study of close to 300 patients, found that psychiatric diagnosis was not a risk factor. In terms of severity of tardive dyskinesia, Glazer and Morgenstern (1988) discovered that patients with affective disorders had a more severe form of tardive dyskinesia. To summarize, although there is some literature suggesting that affective disorders may be a risk factor for developing tardive dyskinesia in patients exposed to typical antipsychotics, the findings are not compelling. Another consideration is to consider outcome as the severity of tardive dyskinesia rather than the relative risk of developing the condition. In this regard it is possible that patients with affective disorders who may develop tardive dyskinesia may be more incapacitated. Nonetheless, with the availability of other compounds such as lithium, anticonvulsants, or the atypical anti psychotic agents, the use of typical antipsychotics in affective disorders needs to be clearly justified. The superiority of the atypical agents also includes a more benign adverse effect profile with a lower risk of extrapyramidal side-effects, lower risk of tardive dyskinesia, lower risk of hyperprolactinaemia, and lower risk of anticholinergic side-effects. In addition to safety concerns the atypical agents appear to have a wider therapeutic spectrum in patients with schizo phrenia. Tohen agents, due to an affinity to serotonin and norepinephrine receptors, may have mood-altering properties. Clozapine Reports of the efficacy of clozapine in bipolar and schizoaffective disorder first appear in literature in the early 1970s (Faltus et al. A number of publications have found clozapine to be highly effective in the treatment of bipolar disorder. However, the vast majority of those studies have been case reports or open-label trials. The authors identified a limited number of controlled studies that included patients with psychotic mood disorders or schizoaffective disorders. Of note, a double-blind com parison study was recently published by Barbini et al. The authors concluded that patients receiving clozapine had a faster onset of action than those receiving chlorpromazine. The difference was statistically significant at the first assessment at week two, and remained significant at week three. The review included two double blind studies, eight open-label, 10 retrospective studies and 10 case reports. Of those 30 studies, 10 provided information that enabled the authors to estimate an overall assessment of the efficacy of clozapine in terms of the percentage of patients responding to clozapine (McElroy et al. Of those 10 studies a total of 350 patients with psychotic mood disorders were treated with clozapine; of which these patients had a bipolar disorder and 221 had a schizoaffective disorder in the bipolar phase of the illness. When those patients were compared with schizophrenic patients in seven of the 10 studies (n = 692), the response of the schizophrenic patients was 61. The first one, conducted by Calabrese and colleagues (1996), reported Antipsychotics in acute mania 379 the use of clozapine in 25 patients with acute mania, non-responsive to lithium, valproate, and typical antipsychotics. Criteria for non-response included the use of lithium carbonate at a blood level of 0. In addition, patients were required to have a history of not responding to a 6-week trial of a typical antipsychotic at a dose equivalent of 20 mg of haloperidol. The authors found that, in 22 of the 25 patients who completed the trial, 72% (18) had a marked improvement, and statistical significance was attained in the first week of treatment. A similar study, conducted at McLean Hospital (Tohen and Zarate 1998), included 24 patients who had a previous history of failing to respond to typical antipsychotics (chlorpromazine 500 mg or equivalent or lithium 0. Fifteen patients were able to complete this 13-week trial, of whom 87% were classified as very much or much improved. In the Young Mania Rating Scale a 50% improvement was achieved in 93% of the patients. The studies conducted by Calabrese and colleagues, and at McLean Hospital, suggest that clozapine may be effective in treatment-resistant manic patients. Although the efficacy of clozapine in acute mania appears convincing, less evidence is available for its effects as a mood stabilizer. After the patients were treated with clozapine the mean number of hospital izations was 0. In another report by Suppes and colleagues (1999), there was a significant improvement in psychotic and affective symptoms 6 months after being randomized through either clozapine or usual treatment. In a retrospective review that included 52 patients with bipolar disorder, 81 with schizoaffective disorder, and 14 with psychotic depression, the authors found that psychotic mania and schizoaffective bipolar patients had significantly better outcomes than patients with psychotic depression or schizoaffective-depressed type; suggesting that the index episode of mania or schizoaffective bipolar type predicted a better outcome. In addition, patients with a psychotic affective disorder had a better outcome in social 380 M. Tohen functioning compared to 40 patients with schizophrenia who were followed as a comparison group. A number of other case reports have also suggested that risperidone has mood-altering properties (Hillert et al. Similarly, Keck and colleagues (1995), in a retrospective chart review, found that patients with bipolar disorder or schizoaffective disorder depressed type had a good response when risperidone was added to mood stabilizers. The investigators studied 45 patients in a 4-week trial random ized to up to 6 mg of risperidone, up to 10 mg of haloperidol, and lithium 800�1200 mg daily, with blood levels 0.
Discount 500mg biaxin free shipping. Gastritis Diet Secrets! Banish Gastritis forever with this Gastritis Diet!.