

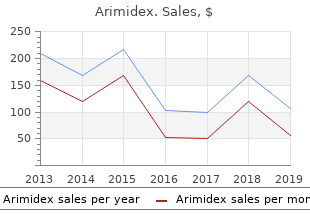
Arimidex
"Buy arimidex with mastercard, workout tips women's health."
By: Randolph E. Regal, BS, PharmD
- Clinical Associate Professor, Department of Clinical Pharmacy, College of Pharmacy, University of Michigan
- Clinical Pharmacist, University of Michigan Health System, Ann Arbor, Michigan

https://pharmacy.umich.edu/people/reregal
The rapid component is in the lesions cause coarse nystagmus towards the side of the direction of gaze pregnancy videos giving birth purchase 1mg arimidex with mastercard. The fundamental cause is probably quite lesion and fne nystagmus to breast cancer jackets purchase arimidex once a day the opposite side menstrual cycle day 8 discount generic arimidex uk. Nystagmus different from that of true nystagmus pregnancy 8 weeks 3 days arimidex 1 mg fast delivery, although both may may also occur in adults as an occupation neurosis, the occur together. Nystagmus may be congenital or early infantile, or Types and Clinical Features it may be acquired. These two groups of cases should In congenital and early infantile nystagmus the patient be carefully distinguished on account of their different is wholly unaware of the movements, since objects do not pathological foundations. To-and-fro movement is noticed by parnystagmus dating from birth or within a few weeks of ents or relatives. Vision is usually defective in spite of birth occurs in congenitally malformed eyes, in albinism, correction of errors of refraction which generally accomand in eyes with congenital or early acquired opacities pany the defect. Visual symptoms of oscillopsia are usually of the media (such as leucoma or cataract) or macular absent when the onset is less than 8 years of age. The cause in these cases is inability to develop cases of acquired nystagmus in adults, objects appear normal fxation. Oscillopsia is the perception of the frst few weeks of life, the eyes being moved aimlessly the environment appearing to oscillate horizontally, vertiand independently before it is acquired. Others may complain of blurred or tive at this period seriously diminishing the acuity of unstable vision. Nystagmus is present cases the movements are very fne and not easily detectin most cases of total colour blindness in which vision is able. In such cases it may be necessary to examine the eye carried out by the rods alone, and there is therefore a cenvery carefully with an ophthalmoscope because the prestral scotoma. In some congenital cases it is impossible ence of nystagmus can be demonstrated in the magnifed to discover any cause. This form occurs in the frst mus can be slow, fast; fne, coarse; horizontal, vertical, year of life as spasmus nutans, in which it is associated rotatory, mixed; jerky (slow drift in one direction as slow with nodding movements of the head. The nodding of the phase followed by an abrupt return to normal position by head may be anteroposterior (affrmation), lateral (negafast phase, cyclic pattern) or pendular (drift occurs in two tion) or rotatory. It develops some weeks before the nysphases of equal speed with a smooth back-and-forth movetagmus, ceases during sleep, and disappears before the ment of the eye). The nystagmus is very fne and rapid, and may In latent nystagmus no movement is present when both be vertical, rotatory or lateral and is generally more eyes are open but nystagmus is elicited only when either marked in one eye. The fast phase of nystagmus beats towards pears in time?one of the few cases in which nystagmus the viewing eye. The nystagmus may disappear in alternating sursumduction or dissociated vertical deviaone eye before the other; such cases may be mistaken for tion characterized by either eye slowly elevating with an true unilateral nystagmus. This may nystagmus is congenital and hereditary, a condition which occur spontaneously when the patient is tired or day-dreampersists throughout life. The deviation is usually Nystagmus blockage syndrome is a specifc type of bilateral but may be asymmetrical. Manifest latent nystagdisorder where nystagmus decreases when the fxating eye is mus occurs in children with strabismus or decreased vision in adduction and patients demonstrate esotropia to dampen in one eye, in whom the non-fxating or poorly seeing eye the nystagmus. When either eye is covered, the There are some important types of nystagmus with lonystagmus increases. They are not uncommon in normal people in called see-saw nystagmus of Maddox, this is a disjunctive certain conditions such as fatigue. It is classically considered as a sign of parachiintoxication, sedatives (barbiturates), cerebellar or brainasmal disease and the lesion usually involves the chiasma or stem disease. Gaze-paretic nystagmus: this has a frequency of 1?2 Convergence and retraction nystagmus: these are beats/second and the eye tends to return to the primary two special forms found with neurological damage localposition with the slow phase of the nystagmus. On attempted upgaze, tagmus disappears completely when total gaze paralysis the eyes display convergence-like movements accompanied occurs. It is common in brainstem to a pineal gland tumour or other mid-brain abnormalidisorders at the pontine level. In young pais in one direction for 60?90 seconds, then the reverse tients, retraction nystagmus should suggest the diagnosis of direction for 60?90 seconds. It may be congenital or acquired and it may be features of the Sylvian aqueduct syndrome consist of: caused by blindness, or by lesions at the cervicomedullary junction. Retraction (and/or convergence) nystagmus Vestibular or labyrinthine nystagmus: this may be 2. Difficult voluntary vertical gaze (especially upward deafness, vertigo, tinnitus and may be due to disease affectgaze) ing the vestibular end-organ (inner ear), eighth cranial 4. Destructive lesions produce a fast phase ments than on command (with an intact Bell phenomenon) opposite to the affected end organ or nerve. Adduction movements with attempted vertical gaze sions produce fast phase in the same direction. Labyrinthine nystagmus occurs in disease of the targets internal ear in which the semicircular canals are involved, 8. Pupillary abnormalities (light-near dissociation), and and can be produced in normal subjects by rotation in a 9. The movement to the opposite side may be induced by syringcommonest site of the lesion is the vermis of the cerebellum ing one ear with cold water, mimicking a destructive lesion or the brainstem when nystagmus is present in the primary or to the same side with warm water (remembered by position. Vertical gaze upwards may be induced by syringing both Downbeat nystagmus: the fast phase is downwards, ears with cold water and vertical conjugate gaze downand indicates posterior fossa dysfunction often at the forawards induced by syringing both ears with warm water men magnum level. When the gaze is returned to the canals can also be stimulated by rotation with the head in a primary position, the fast phase increases in the direction suitable position. Destruction of one labyrinth causes rhyththe eye takes in returning to the primary position. Cerebelmic nystagmus towards the opposite side, which ceases if lar lesions are the most common cause. Gaze-evoked nystagmus: In gaze-evoked nystagmus Miners nystagmus: this occurs chiefy in those who there is no movement of the eyes in the primary position have worked for a long time at the coal face. The nystagmus is essentially rotatory develops with its rapid phase in the direction of gaze and and very rapid; in latent cases it is elicited by fxing the increases when looking in the direction of the fast phase. In severe cases, the this builds to a maximum intensity in the extremes of lids are nearly closed and the head is held backwards; there conjugate gaze and is well sustained. The frequency of the eyes look to the side and is absent in the straight-ahead disease varies inversely with the illumination in the mine, position. The frequency is slow (3?8 beats/second on an suggesting that fxation diffculties in the dim illumination electronystagmogram). Improvement in Therapeutic modalities available to manage nystagmus miners lamps and in the lighting of mines eliminated the include optical aids such as spectacles, prisms and contact disease. There are a number of ocular motility disorders, which Whenever possible, the underlying aetiology must be occur in childhood and resemble nystagmus. Periodic alternating includes ocular bobbing, futter-like oscillations of the eyes, nystagmus may respond to baclofen (5 mg orally thrice ocular dysmetria, opsoclonus, ataxic conjugate movements daily increased gradually by 15 mg/day every 3 days until of the eyes and ocular myoclonus. Baclofen is not recommended In ocular bobbing the eyes remain motionless in the for use in children. Acquired pendular nystagmus is known primary position and then suddenly the eyes deviate downto respond to gabapentin. Refractive errors must be corwards or, less commonly, upwards after which they slowly rected, preferably with contact lenses, and amblyopia return to the primary position. Attempts have characteristically have loss of caloric responses on coldbeen made to convert the movements of a nystagmus into water irrigation of the ears with total horizontal conjugate audible stimuli, which can be heard by the subject who uses gaze palsies. They usually have a massive neoplastic lesion this feedback signal to control the nystagmus by maintaininvolving the pontine brainstem and the prognosis is ing a constant tone. Nystagmus in the primary position of gaze remains Flutter-like oscillations of the eyes and ocular dysmeta particularly troublesome disorder, which is relatively ria are ocular signs of interruption of cerebellar connections refractory to medical intervention. They represent the dysmetric overshoots downbeat nystagmus seen in lesions of the posterior fossa. Patients have a clear slow phase of the nystagmus and this effect may improve sensorium; the disorder often follows an episode of benign visual acuity, unless there is some other cause for the lowencephalitis and usually has a good prognosis. Oculopalatal myoclonus is an unusual disorder in Indications for surgery are visually disabling nystagmus which the patient develops associated movements of the with excessive excursions or a null point in extreme lateral eyes, palate, face, platysma, larynx, eustachian tube orifce, gaze, in which the patient has to maintain an uncomfortable tongue and occasionally the extremities. The basic aim of brainstem damage in the myoclonic triangle, which has as surgical treatment is to transfer the neutral point (where its boundaries the red nucleus above, inferior olive below the nystagmus is least apparent) from an eccentric position and dentate nucleus of the cerebellum posteriorly. It occurs to a straight-ahead position so that there is an elimination most commonly in association with vascular disease or as a of the compensatory head posture.
R551 menstrual funny cramps jokes purchase arimidex 1mg otc, E832 and E831 include the palmar and digital components of the Dupuytrens procedure women's health clinic in oregon city discount arimidex 1 mg otc, when rendered women's health big book of yoga pdf order 1mg arimidex free shipping. E497 is payable in addition to women's health issues in thrombosis and haemostasis 2015 best purchase arimidex R322 and R345 if a pedicled vascularized bone graft is used in addition to, or in place of a non-vascularized bone graft. F019 and Z279 rendered in conjunction with R322 and R345 are not eligible for payment. An elbow procedure listed in the Elbow section of the Schedule performed arthroscopically is eligible for payment in addition to R683 if that procedure is not described as a component of R683 or described by an E-add-on code to R683. Arthroscopic E-add-on codes listed below are not eligible for payment in addition to R683 when the service described by the E-code is a generally accepted component of a procedure described in Note #1. A shoulder procedure listed in the Shoulder section of the Schedule performed arthroscopically is eligible for payment in addition to R684 if that procedure is not described as a component of R684 or described by an E-add-on code to R684. Arthroscopic E-add-on codes listed below are not eligible for payment in addition to R684 when the service described by the E-code is a generally accepted component of a procedure described in Note #1. Midface fractures Application of craniofacial suspension wires and external fixation devices (not to be billed in addition to maxillary repair). Z239, Z240, R652 or D062 are not eligible for payment in addition to F138 or F139. A knee procedure listed in the Knee section of the Schedule performed arthroscopically is eligible for payment in addition to R687 if that procedure is not described as a component of R687 or described by an E-add-on code to R687. Arthroscopic E-add-on codes listed below are not eligible for payment in addition to R687 when the service described by the E-code is a generally accepted component of a procedure described in Note #1. R687 is an uninsured service for arthroscopic lavage of the knee alone (without debridement) for osteoarthritis. Arthroscopic lavage of the knee alone (without debridement) is not recommended for any stage of osteoarthritis. E489 and/or E494 are not eligible for payment in addition to E496 for debridement of attachment site. R695, R696, and R697 include any neurovascular exploration and/or protection and tenolysis, when rendered. An ankle procedure listed in the Foot and Ankle section of the Schedule performed arthroscopically is eligible for payment in addition to R688 if that procedure is not described as a component of R688 or described by an E-add-on code to R688. Arthroscopic E-add-on codes listed below are not eligible for payment in addition to R688 when the service described by the E-code is a generally accepted component of a procedure described in Note #1. Services listed under "Skin Flaps and Grafts" are not eligible for payment with R549 or R576. R576 and E831 include the plantar and digital components of the Dupuytrens procedure, when rendered. F063, F065) may be eligible for payment when rendered in addition to D026 or D028. Identification of the anatomy of the paranasal sinuses distorted by previous surgery, trauma, abnormalities of development or benign or malignant tumours; or 2. A pathological lesion abuts the base of the skull, orbit, optic nerve or carotid artery. When bronchoscopy, flexible or rigid, is rendered in conjunction with laryngoscopy or oesophagoscopy, only the bronchoscopy is eligible for payment. Bronchoscopy rendered by the same surgeon immediately following thoracic surgery under the same anaesthetic is not eligible for payment. Bronchoscopy (including intraoperative bronchoscopy) rendered the same day as a major lung resection is not eligible for payment if a bronchoscopy has been rendered by the same physician to the same patient in the 3-week period preceding the major lung resection. Z360 is eligible for payment only for life-threatening emergency situations where the patient is not intubated. Life Threatening Critical Care and Other Critical Care services are not payable in addition to Z360 to the same physician for the same patient, same day. Z325 is eligible for payment only for life-threatening emergency situations where the patient is not intubated. Percutaneous tracheostomy, cricothyroidotomy or other emergency airway punctures do not constitute Z325. Z361 and Z362 are not payable for adjustment of a previously inserted indwelling pleural catheter. Unless otherwise stated, excision or repair procedures for arteries and veins include endartectomy, thrombectomy and/or bypass graft. Excision or repair procedures for arteries and veins include harvest of graft tissue, except where harvest of graft tissue is explicitly excluded from the procedure. Where harvest of graft tissue is included as a specific element of the procedure, the harvest is an insured service payable at nil. The basic anaesthetic fee of 28 units or more for major cardiovascular surgery includes such procedures as insertion of C. Re-operation involving open heart procedures with pump # E670 following previous thoracotomy. R701 or R702 are eligible for payment only for paracorporeal devices inserted for less than 14 days. Despite payment rule #1, R701 is also eligible for payment in addition to R703 or R704 when a right ventricular assist device is inserted to support a left ventricular assist device, regardless of the duration of insertion of the right ventricular assist device. R703 is eligible for payment only for paracorporeal devices inserted for 14 or more days. R705 is only eligible for payment for removal of paracorporeal or implantable ventricular assist devices inserted for 14 or more days. Z744 (decannulation of circulatory assist device) is eligible for payment for removal of paracorporeal or implantable ventricular assist devices inserted for less than 14 days. Only one of Z744 or R705 is eligible for payment per patient per day for removal of ventricular assist devices. Extracorporeal membrane oxygenator procedures do not constitute R701, R702, R703 or R704. If a ventricular assist device is replaced, both the appropriate removal and insertion fee codes are eligible for payment. For the anaesthesiologist, when off-pump coronary artery bypass grafting is rendered, submit claim using E645C with 40 basic units plus time units, instead of R742C or R743C. For the surgical assistant, when off-pump coronary artery bypass grafting is rendered, submit claim using E645B with 24 basic units plus time units, instead of R742B or R743B. Where a single segment of vein is used for more than 2 anastomoses, the second and subsequent anastomoses are to be claimed at 50% of the E654 fee. Percutaneous transluminal catheter assisted closure for Secundum arterial septal defect Z465 device closure of a single defect. R784, R785) includes repair to the profunda femoris artery as far as the first major branch. If the repair extends beyond the first major branch of the profunda femoris artery, R815 may be claimed in addition. If the repair extends beyond the second major branch of the profunda femoris artery, R856 instead of R815 may be claimed in addition. For procedures involving the application of a complete aortic cross clamp, the anaesthetic basic fee will depend on: a. These services include insertion of all catheters including access catheters, interpretation of any images which may be taken at the time of the procedures. E510 is not eligible for payment for branched or fenestrated devices to the common iliac artery(s). Endovascular repair for abdominal aortic aneurysms is only recommended for patients who are at high-risk of perioperative morbidity or death from open surgical repair. Abdominal aorta repair or excision with graft # R802 aneurysm repair alone or including unilateral common femoral repair. R878 is not eligible for payment same patient same day as R809, R791, R794, R787, R780 or R797. R879 is not eligible for payment same patient same day as R783, R784, R785, R860 or R861. Obtaining and interpreting any images in conjunction with R878 and R879 are not eligible for payment to any physician. Bilateral procedures for R878 or R879 are payable only as separate services when subintimal dissection is performed using separate bilateral incisions.
Inferior oblique Sherrington law of reciprocal innervation: During the Inferior rectus initiation of an eye movement menstrual cup reviews cheap arimidex online mastercard, increased innervation to menopause zest generic arimidex 1mg otc an extraocular muscle is accompanied by simultaneous inhibiSuperior oblique tion (a reciprocal decrease in innervation) of the direct antagonist of the contracting muscle of the same eye pregnancy genetic testing discount 1mg arimidex. Note: the diagram shows the various subnuclei but is not directly representative of the actual location; for example menopause relief without hormones purchase cheap arimidex line, a is in reality a single, central, caudally located nucleus. Their action is coordinated by is composite and divided into cell masses or subnuclei subintermediate centres situated in this region by which serving the individual extrinsic ocular muscles, as is seen in refex activities are governed. A single, central, caudally located nucleus innercentres are linked with the vestibular apparatus whereby vates both levator palpebrae superioris muscles. Paired they become associated with the equilibration refexes bilateral subnuclei that innervate the superior recti have and the cerebral cortex so that voluntary movements and crossed projections that pass through the opposite subnuparticipation in the higher refexes involving perception cleus and join the nerve of the opposite side. Paired the oculomotor, or third cranial nerve, supplies all the bilateral subnuclei with uncrossed projections innervate the extrinsic muscles except the lateral rectus and superior medial recti, inferior recti and inferior oblique muscles. It also supplies the sphincter pupillae and ciliary Parasympathetic input to the sphincter muscle of the iris muscle. The superior oblique is supplied by the trochlear and ciliary body arises from the single Edinger?Westphal (fourth) nerve and the lateral rectus by the abducens nucleus. A bilateral third nerve palsy without ptosis informs a large, continuous mass of nerve cells situated near dicating sparing of the single levator subnucleus and a the midline in the foor of the aqueduct of Sylvius beneath unilateral third nerve palsy with contralateral superior recthe superior colliculus (Fig. The cells nearest the tus involvement and bilateral ptosis are both indicative of midline towards the anterior part of the third nucleus are obligatory nuclear involvement. Unilateral ptosis, unilateral smaller than the others: they form the Edinger?Westphal internal ophthalmoplegia and unilateral external ophthal(and Perlia) nucleus which supplies fbres to the ciliary moplegia with normal contralateral superior rectus function muscle (accommodation) and sphincter pupillae (constricare conditions that exclude a nuclear lesion. Chapter | 25 Anatomy and Physiology of the Motor Mechanism 409 the fourth nerve nucleus is located more caudally F? Nearly, if not quite, all the fbres decussate in the superior medullary velum and are distributed to the superior oblique muscle of the opposite side. The sixth nerve nucleus is situated much further caudally in the brainstem (Fig. Hence, vascular and other lesions of the sixth nucleus are very liable to be accompanied by facial paralysis on the same side. All the fbres of the sixth nerve are distributed to the ipsilateral lateral rectus. So long as the fixation point (F) is imaged on are also interrelated through this bundle so that coordinaeach macula, the fixation reflex maintains the posture of the eyes steady tion of the two eyes is maintained. If, however, F is tant among such connections is the group of fbres which moved to F, the retina on the right of the macula is stimulated and sets up a refixation reflex. The afferent path is: (a) retinae n optic nerve n chiasma n right optic tract; (b) lateral geniculate body n right optic radiations n striate area of occipital cortex; (c) peristriate occipital cortex. In the present case, acting essentially through the left sixth nerve and the branch of the right third nerve to the medial rectus, the muscular tone is altered (hollow arrows) to Centre for conjugate lateral orientate the eyes so that F again falls on each macula. The frontal cortex has an area which controls quick fxational eye movements to the opposite side. Both supranuclear areas send the abducens nuclei and the oculomotor nuclei by way of the medial impulses to the brainstem to the centres which control conlongitudinal fasciculus. The centres controlling eye movements in the fbres control conjugate movements, vertical and horizonbrainstem are the fnal common pathway conveying imtal, of both eyes; movements of individual muscles are not pulses for movement in a particular direction, irrespective represented in the cortex. Stimulation of the cortex or the of whether the movement is voluntary or involuntary, a sactracts unilaterally therefore produces horizontal conjugate cade or a pursuit, or a vestibular refex eye movement. These pathways are tested clinically and it controls conjugate horizontal movement to the by asking the patient to look to the right, left, upwards or ipsilateral side. A destructive lesion in the right prefrontal lobe An area controlling vertical movements lies just above would lead to an inability to look conjugately to the left. Vertical movethe centre for convergence (Perlia nucleus) is associated ments are generated by bilateral simultaneous stimuli from with the third nerve nucleus and lies in the region of the both sides. All refexes is the visual pathway; the efferent runs down voluntary movements are initiated by the cerebral cortex the optic radiations to the posterior longitudinal bundle which sends impulses to the specifc centres for a particular (Fig. The cerebral cortex represents a movepathways are tested by asking the patient to follow an object, ment of gaze involving both eyes and not individual muswhich is passed horizontally and vertically so that the concles. If a lesion affects an individual muscle or group of jugate following movements of the eyes may be elicited. An elaborate system of statokinetic refexes coordinates Voluntary ocular movements are initiated in the pyrathe position of the eyes when the head is moved in space; midal cells of the motor area of the frontal cortex in their afferent path runs from the semicircular canals of the the second and third frontal convolutions of both sides inner ear to the mid-brain centres. The fbres enter the knee of the internal capmovements of both eyes, a slow tonic movement in the sule as part of the pyramidal tract close to the fbres governdirection of equilibration and a quick return (nystagmus). If the chin is depressed the eyes normally elevate if fxation is maintained, and if the head is rotated on a vertical axis the eyes maintain fxation as a result of the statokinetic refexes. These movements are often referred to as doll?shead movements and they may be selectively maintained when voluntary and saccadic conjugate gaze and pursuit (following) conjugate gaze are disturbed as in the Sylvian aqueduct syndrome (see Chapter 31, Diseases of the Nervous System with Ocular Manifestations). Optokinetic movements are initiated by rotation or movement of the environment or the visual target. A tentative localization of the ments of the eyes in respect to movements of the head upon main ocular motor areas in part transferred from the brain of primates the body. It is to be noted that the apparently accurate localization pulses from the neck muscles, which are linked with the of certain areas is by no means factual or constant. Points on the two retinae, which are Fixation and Projection not corresponding points in this sense of the term, are We have already seen that the location of the image of an called disparate points, and if an object forms its retinal external object on the retina is determined by a line passing images on these, it will be seen double (binocular diplopia). ConIf the disparity is slight there is a tendency to move the eyes versely, an object is projected in space along the line passing so that the images may be fused by means of the fusion through the retinal image and the nodal point. When a distant object is looked at the visual axes are practically Fixation, Fusion and Refex Movements parallel; the object forms an image upon each fovea centralis. Since the most accurate vision is attained by the foveae it is necessary that the eyes be rapidly orientated so that the imCorrespondence age of an object of interest falls upon them or that of a Any object to one side of the fxation target forms its retinal moving object be retained on them. This ascendancy of the images upon the temporal side of one retina and upon the foveae is maintained by the fxation refex (Fig. The peristriate, posterior temporal both eyes horizontally in opposite directions. The system and dorsal prefrontal cortex are regions is required to maintain foveal position of the image of an which send convergence and divergence object which may be moving away or towards the observer impulses or may be located near or far away Fixation Maintaining the image of the object of regard on Supplementary eye feld maintains fxation the fovea with the eyes in specifc orbital locations and also inhibits visually evoked saccadic refexes. The frontal eye feld is involved in changing fxation (disengaging) VestibuloPrevents slipping of the retinal images when the head Otolith receptors and semicircular canals. If an object is being nuclei pursued with eye and head movement, vision cancels the vestibulo?ocular refex to prevent the eyes from moving in the opposite direction as the head Optokinetic During prolonged rotations the optokinetic system Direct pathway in the brainstem and indirect movements sustains compensatory eye speed at the same speed as pathway involving the brainstem, cerebellum the head. Optokinetic nystagmus is evoked during head and cerebral hemispheres, parts of the striate motion with the environment stable and with the head still, and extrastriate visual cortex, parietal, but the visual image in motion. If the target is small and posterior temporal, prestriate and lateral attention voluntarily guided, smooth pursuit is induced occipital cortex followed by opposite quick phases. Each frontal eye feld or superior colliculus can generate horizontal saccades to the opposite side. Vertical saccades are generated by simultaneous stimuli from bilateral frontal eye felds or superior colliculi. The object moves outside the binocular feld of vision and the strongest prism whose deviating effect can be tolerated eyes then refxate on another object. The activity of this without developing diplopia or double vision is a measure refex is demonstrated by the rapid to-and-fro movements of the refex fusional capacity (Fig. A prism bar of the eyes of a person watching passing objects such as consists of a battery of prisms of increasing strength and is trees or electric poles while looking out of the window of a a convenient instrument in clinical testing (Fig. The latter phenomenon can be used as a test to demonstrate the In view of the distance between the two eyes, it is obvious integrity of the refex paths. If the object is a solid body the right eye may be demonstrated clinically by placing a small prism in sees a little more of the right side of the object, and vice front of one eye while the patient regards a distant light. The images of the fixation point (F) fall on each fovea (f); those of an object near the eye (T) will fall on t, giving rise to crossed diplopia. It will thus be found that near objects suffer a crossed (heteronymous) diplopia; distant objects an uncrossed (homonymous) diplopia. This diplopia is physiological and is perceptually suppressed in actual vision, but produces a psychological impression, which is translated into appreciation of distance. It follows that accuracy of stereoscopic vision depends upon good sight with both eyes simultaneously.
Thus menopause uptodate buy arimidex 1 mg, fngerprint experts may have diffculty when asked to pregnancy kicking purchase 1mg arimidex mastercard make judgments that depend in 15 the women's health big book of exercises pdf download discount arimidex master card. The part on differences that exist in the noise dimensions menstrual vertigo best order for arimidex, which previous section describes how the psychological work on presumably they have learned to ignore. There may appear to be a gulf between similarity judgBurns and Shepp (1988) measured the similarity relations ments, which one may think of as a continuous measure, between color chips. They found that although novice and the type of decision arrived at by latent print examinobservers tended to treat the dimensions of hue, saturaers. The language may be different in various jurisdictions, tion, and brightness as integral, experts were more likely to but typically examiners testify that two prints either came differentiate these dimensions. Goldstone (1996) extended from the same source or did not come from the same this work to show that people who learn a categorization source. They may or may not attach some kind of confbecome sensitized to the relevant dimensions. This might suggest that the rization work described above suggests that experts learn similarity literature may have little to do with latent print to separate out the relevant dimensions, which helps them examinations. However, the authors of this chapter would more accurately gauge the similarity of two objects. No two prints are ever of face recognition, which reveals not only the nature of identical; therefore, the task always requires some element the dimensions of faces but also provides a psychological of comparison and similarity computation. Examiners then space that can be used to make predictions for memory translate this to a categorical judgment, presumably using experiments. A psychological space is an abstract represome rule such as: These two prints are more similar to sentation that places more similar faces close together each other than any other close non-match that I have ob(Valentine, 1991). Busey (1998) gathered a large set of served or The two prints are suffciently similar that I can similarity ratings between all possible pairs of 104 faces. Here, the focus is table but was then used to make predictions for memory on the cognitive processes, which result from comparing experiments (Busey and Tunnicliff, 1999). The way fngerprint examiners Steyvers and Busey (2001) demonstrated the matches and explain their conclusions, and the way they express their mismatches between a physical representation computed decisions, may vary from one place to another and may from images and psychological spaces computed from change over time; however, the cognitive processes that similarity ratings. In part, the differences come from the are the focus of this chapter remain the same. What emerges from Phenomena this summary is a view that the human visual system is remarkably good at extracting the structure that exists in a Although the active and dynamic nature of cognition is class of stimuli. This learning process occurs with very little the basis of intelligence and expertise, it also introduces conscious direction beyond the initial selection of relevant a multitude of elements that make humans vulnerable features. All that is required is a constant set of example to distorting information and thus making errors (Dror, in stimuli that provide the kinds of statistical regularities press). This section elaborates and illustrates how human what are the relevant features required for the task. This is information processing can distort information in a variety not to imply that this is an easy process; in fact, the feld of ways. The next section shows how these phenomena should argue for more hours of training to provide the large relate to fngerprint identifcation. Although the two black shapes by developing scientifc-based training and utilizing technolabove, in Figure 15?6, are identical, they are perceived ogy (see Dror, Stevenage, and Ashworth, 2008). The active and Experts often ask the question, how much matching infordynamic nature of the perceptual system not only has the mation is enough? The perceptual learning literature does potential to distort the incoming data, as already illustrated, not provide a direct answer, but the tools from cognitive but it can also add information and make us perceive things science illustrate how different factors trade off. For example, in Figure 15?7, one next section, a computation modeling approach is used to perceives imaginary subjective contours making a white address the relation between quantity and quality. Furtherquality could be measured in several ways but, in general, more, this imaginary white square incorrectly seems to it represents the degree of visible print information relative be of a different shade than its surroundings (compare the to the amount of noise caused by dust or other artifacts shade in points A and B, which are in fact identical). Image quantity reprethese examples demonstrate that even the lower level sents the surface area of usable print information, which sensory mechanisms are not passive or isolated from a could be measured in units of ridge widths or square cenvariety of factors that can affect and distort what is pertimeters. Thus, much of what is perceived, even at the as going together, in principle it is possible to separate the lower level mechanisms, is dependent on the perceiver two factors. De facto, they disregard the context is not provided by the environment but rather and miss possibly critical information in an image. Because of these as well as other cognitive mechanisms, At a more scientifc level, this can be demonstrated by the same visual image can, in fact, get different interpretashowing that interpretation of the central image in Figure 8 tions depending on the context in which it is presented. Rather than manipulating the external context of A, as the letter B or as the number 13?; either can be B, C vs. If the central imwith the vertical contextual information or B with the age is presented in a context that motivates people to see horizontal contextual information). For example, one role in how people process information, here too they are can be highly affected by states of wishful thinking, cognisubject to vulnerabilities. In fact, the mind can play many tive dissonance, escalation of commitment, or confrmation tricks and cause a wide range of phenomena. In these cases, the collection and interpretation of mon saying that love is blind is a refection of this effect. It is obvious that fngerprint experts, like experts in other Again,even if the decision-maker comes initially with no domains and nonexperts in everyday life, are susceptible preconceived decisions or biases, as decisions are considto perceptual, cognitive, and psychological phenomena. It is important As already illustrated, these processes are highly depento consider which ones are relevant, and how. For example, dent on psychological elements and processes rather than if fngerprint identifcation requires comparing the length purely on the relevant information. In Figure 15?9, the top horizontal line is perceived how information is collected, processed, and interpreted as shorter than the bottom horizontal line, although the two. This is a demonstration of some potential psychological and cognitive phenomena that may be directly related to fngerprint identifcation. Other scientifc investigations have been Psychological Elements in conducted to directly address fngerprint identifcation. A whole range of perceptual, cognitive, and psychological elements play an A number of research studies have examined the possible integral role in all the stages of the identifcation process: infuence of context on decisions about whether fngerfrom fnding and collecting prints, perceiving them, and prints match or not (see, for example, Langenburg et al. In the sections Charlton, 2005; Dror and Charlton, 2006; Dror, Charlton, below, psychological and cognitive phenomena are tied toand Peron, 2006). In one study (Dror, Peron, Hind, and gether and related to the world of fngerprint identifcation, Charlton, 2005), pairs of fngerprints were presented to and research that directly examines the fngerprint domain nonexperts. Finally, some practical implications and some were clearly not a match, and others were ambiguapplications of these elements are discussed. Then, prior to the participants examining the fngerto move forward and enhance fngerprint identifcation can prints, contextual information about the crime at issue only be achieved once we are willing to accept that these (including photos from the crime scene) was presented. To collect ecologically valid and robust data, Dror and CharlHowever, the other half of the prints were presented within ton (2006) and Dror, Charlton, and Peron (2006) employed a highly emotional condition, with photos that were sciencovert data collected from fngerprint experts during their tifcally proven to provoke emotional reactions (Lang et al. A within-subject experimental design was 1995), such as the photograph in Figure 15?10. The results of the study showed that emotional context and this is a very robust and powerful experimental paradigm, mood affected how fngerprints were matched. This not only the effect of emotional context was dependent on the diffprovides more meaningful and interpretable data, but each culty of making the match. Furthermore, this affected matching decisions when the pairs of fngerprints allows the researcher to isolate, focus on, and examine the were ambiguous and there was not enough data to make contextual infuences themselves rather than revealing posa clear and simple identifcation or exclusion decision. However, approximately 5 years earlier as a clear and defnite match emotional experiences do seem to play a role in the work or exclusion. In In these studies, the very same pairs of fngerprints were fact, even in the normal working environment, experts bere-presented to the same experts, only now they were prehave differently if they know they are being observed, taksented within an extraneous context that might bias them ing part in research, or being tested. A control condition includwants to test and examine how people drive, then examined pairs of prints that were presented without manipulating their driving during an offcial driving test, or even when ing the context. In these two studies, a total of 53 pairs of they know they are being watched (or within the range of prints were presented to 11 experienced latent fngerprint a speed camera), will hardly refect how they actually drive experts (none of whom participated in both studies). In a combined meta-analysis of these two experiments (Dror and Rosenthal, 2008), the reliability and biasability of 15?17 C H A P T E R 1 5 Special Abilities and Vulnerabilities in Forensic Expertise the fngerprint experts was analyzed and determined. Eight however, does reinforce the conclusion that as an examiner out of the 11 experts made some inconsistent decisions shifts his or her decision criteria with changes in experithat conficted with their previous decisions on the same ence, care must be taken to avoid shifting them too much. These conficting decisions mainly ocCentral to any shift in criteria must be a set of procedures curred in the more diffcult prints and with prints that were to obtain accurate feedback from know fngerprints, either originally judged as identifcations. However, some inconin the form of formal profciency testing or informal practice sistent decisions also occurred with relatively easy prints working with a community of examiners.
Cheap arimidex 1mg on-line. womens health.