

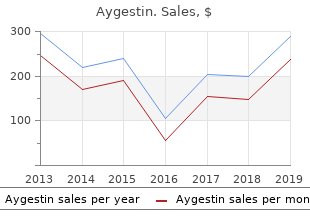
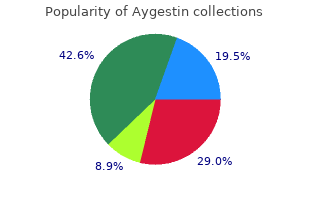
Aygestin
"Generic aygestin 5mg mastercard, menopause relief."
By: Paul Reynolds, PharmD, BCPS
- Critical Care Pharmacy Specialist, University of Colorado Hospital
- Clinical Assistant Professor, Department of Clinical Pharmacy, Skaggs School of Pharmacy and Pharmaceutical Sciences, University of Colorado, Aurora, Colorado

http://www.ucdenver.edu/academics/colleges/pharmacy/Departments/ClinicalPharmacy/DOCPFaculty/Q-Z/Pages/Paul-Reynolds,-PharmD.aspx
Select patients are candidates for a restorative proctocolectomy performed in a single step breast cancer charities generic aygestin 5mg amex. After a temporary protective ileostomy is closed women's health issues symptoms order generic aygestin pills, patients can defecate through their anus pregnancy due date calendar order 5 mg aygestin with visa. Although pouchitis is a complication in 25% of patients women's health clinic andrews afb discount aygestin 5mg overnight delivery, the ileoanal pouch is an acceptable and successful alternative to standard ileostomy. Overview the complications of ulcerative colitis can be divided into those that affect the colon and those that are extracolonic. Toxic Megacolon Overview the most feared complication of ulcerative colitis is the development of toxic megacolon. It occurs as a result of extension of the inflammation beyond the submucosa into the muscularis, causing loss of contractility and ultimately resulting in a dilated colon. Dilation of the colon is associated with a worsening of the clinical condition and development of fever and prostration. Diagnosis this diagnosis is based on radiographic evidence of colonic distention in addition to at least three of the four following conditions: fever higher than 38. At least one sign of toxicity must also be present (dehydration, electrolyte disturbance, hypotension, or mental changes). There may be rebound tenderness, abdominal distention, and hypoactive or absent bowel sounds. However, perforation can also present in severe ulcerative colitis even in the absence of toxic megacolon. Steroid therapy has been suggested to be a risk factor for colonic perforation, but this is controversial. Radiography X-rays of the abdomen reveal colonic dilation, usually maximal in the transverse colon, which tends to exceed 6 cm in diameter. Serial plain abdominal x-rays of the abdomen taken at 12?24-hour intervals are useful in following the clinical course. Medical Therapy the goal of medical therapy is to reduce the likelihood of perforation and to return the colon to normal motor activity. A nasogastric tube is placed in the stomach for suction and decompression of the upper gastrointestinal tract. The use of the rolling technique, during which the patient lies on the abdomen for 10?15 minutes every 2 hours while awake, allows for passage of gas and easier decompression of the dilated colon. Broad-spectrum antibiotic coverage is instituted in anticipation of peritonitis resulting from perforation. Intravenous steroids are usually administered in doses equivalent to more than 40 mg of prednisone per day. Surgical Therapy Colectomy occurs in about 25% of patients and is required in almost 50% of patients with pancolitis. Surgical intervention is undertaken if the patient does not begin to show signs of improvement during the first 24?48 hours of medical therapy, as the risk of perforation increases markedly. Colectomy with creation of an ileostomy is the standard procedure, although single-stage proctocolectomy is done occasionally. If surgical therapy is performed before there is colonic perforation, the mortality is approximately 2%. In cases in which there has been bowel perforation, however, the mortality risk increases to 44%. However, some degree of narrowing may be seen in approximately 12% of surgical specimens. Histologically, strictures present with hypertrophy and thickening of the muscularis mucosa without evidence of fibrosis. Strictures tend to occur late in the course of disease, usually 10?20 years after onset of disease. Most strictures occur in the sigmoid and rectum, with an approximate length of 2?3 cm. Strictures have been associated with malignancy, and biopsy of the strictures is warranted. In fact, in patients with long-standing history of ulcerative colitis, a stricture should be considered potentially malignant. Primary Sclerosing Cholangitis Primary sclerosing cholangitis is a chronic cholestatic liver disease characterized by fibrosing inflammation of extra and intrahepatic bile ducts. Patients may have symptoms of fatigue, pruritis, abdominal pain, fever, or jaundice. This usually appears in men after 10?15 years of very mild, even subclinical, pancolitis, and may necessitate liver transplantation in some patients. Formulation(s) 98% w/w powder for suspension Dosing Regimen Volume administered varies based on clinical condition, and anatomic characteristics. Indication(s) Double contrast examination of the esophagus, stomach and duodenum under fluoroscopic guidance. This type of evidence will be used as support for the finding that barium sulfate enhances structural delineation and provides new clinical information about normal and abnormal structure. Enhanced visualization in a specific clinical setting was considered adequate for the purpose of generalization to the various clinical uses in this anatomic region. They can be divided into positive, negative and neutral contrast agents, depending on the extent of attenuation of the x-ray beam. The contrats is provided by low concentration 1% to 2% weight /volume barium suspensions. The contrast agent is administered orally or rectally, is hypertonic, and may lead to hypovolemia and hypotension due to fluid loss from the intestine. For these reasons, water soluble contrast agents are generally used only in situations that preclude the use of barium sulfate for example in patients with suspected bowel perforation or leak, or likely small bowel obstruction and in whom need for surgery is anticipated. The manufacturer did not provide quality information for any of the clinical studies as they had not supplied the product to the study?s investigators. The chemistry review team concluded that Bracco?s historical products were all comparable to their proposed commercial products. The lack of preclinical pharmacology/toxicology data, does not importantly affect the assessment of the product safety. Barium sulfate is a heavy metal with a high atomic number (Z=56) and a K shell binding energy (K-edge of 37. In this manner various masses such as benign or malignant tumors, ulcers, strictures, diverticula, inflammation or infection, altered motility, displacement and other pathology can be identified. In normal subjects, orally administered barium sulfate is generally excreted within 24 hours. The surgeon relied on the esophageal myotomy for radiographic findings to achalasia. Acceptable Mar;23(3):606-10 consecutive patients who flow of contrast was underwent laparoscopic considered evidence of anterior esophageal myotomy recovery of function. An for achalasia from May 1996 abnormal barium esophagram to August 2007 were reviewed (contrast retention or pooling, from a prospective delayed emptying) led to delay institutional review board in initiation of a diet. Reviewer?s comment the Barium sulfate product or reviewer considered the dosing was not specified. Barium complementary to endoscopy commonly recommended swallow and endoscopy essential in the preoperative endoscopy before laparoscopic allowed the diagnosis of hiatal assessment of laparoscopic antireflux and hiatal hernia hernia in 75% and 98%, antireflux and hiatal hernia surgery. This study prospectively was confirmed in 50% by evaluated 40 consecutive barium swallow and 80% by patients who were tested with endoscopy. Results regarding the presence and the type of hiatal hernia found by barium swallow and endoscopy were correlated with the intraoperative finding as the reference standard. Nawaz M, Jehanzaib M, Khan the objective of this study Of the 115 patients, 80 were K, Zari M. Role of barium was to compare the use of a male and 35 were female meal examination in diagnosis barium meal examination in patients. J Ayub Med the diagnosis of peptic ulcer from 27-75 years with mean Coll Abbottabad. In 6 out peptic ulcer disease were of 30 patients with gastric selected for this study and ulcer had radiological underwent a barium meal evidence of malignant gastric examination. The sensitivity of benign/malignant peptic ulcer barium meal in diagnosing was made by barium meal peptic ulcer was 97%, examinations. The clinical presentation and radiologic findings were compared, to assess the diagnostic accuracy of barium swallow in such patients. Clinical records and radiologic reports of 194 patients with globus pharyngeus, were retrospectively reviewed.
In less than a third of the cases the evaluator recommended safe exchange conditions menstrual rage cheap 5 mg aygestin visa. Also critical is that custody evaluators have an understanding of indicators of ongoing danger and safety provisions that can be incorporated into custody and visitation arrangements breast cancer society cheap 5 mg aygestin fast delivery. Custody evaluators should be screened for knowledge of domestic violence dynamics women's health center jacksonville fl 5 mg aygestin visa, impact on children 40 menstrual cycle buy generic aygestin 5 mg, and risk factors for ongoing abuse. Training should be offered and required not only on domestic violence but also on legal issues related to the evaluator?s role and laws governing the court?s requirements and options regarding custody and visitation in domestic violence cases. The court?s role as trier of fact must not be delegated to mental health personnel appointed to assess parenting capacity. The term was used in cases where a parent had apparently attempted to alienate the child from the other parent but the child was not, in fact, alienated (estranged) from that parent; it was used when the alienation was deliberate and without cause and when it was an unintentional result of the victimized parent?s fear and concern. This research must take into account child estrangement from a parent, identifying the causes of the estrangement and analyzing the court?s response. Importantly, research should investigate the impact on children of custody and viii this document is a research report submitted to the U. Violence and the Family: Report of the American Psychological Association Presidential Task Force on Violence and the Family. The highest risk cases for clinicians who work with children: high conflict divorce/custody cases. Custody Evaluations in Cases of Domestic Violence Chapter 1 Problem and Overview of Project Custody and visitation cases are sensitive, often volatile,? and raise some of the most difficult issues before the courts,? according Judith Kaye, the Chief Judge of the Courts of the State of New York (Report of the Family Court Advisory and Rules Committee to p. When custody is disputed between parents, courts sometimes appoint a custody evaluator to conduct an assessment of the family. The purpose of the evaluation is to help the court determine the custody and visitation arrangements that would serve the child?s best interest, the standard for custody awards in all states (Buehler and Gerard, 1995; Frankel, 2007). If the parties allege domestic violence, the evaluation can become more critical: flawed custody and visitation arrangements could put the child and victimized parent at risk of further psychological and physical harm; the victimized parent may be intimidated into surrendering custody. It has been estimated that as many as 50% of custody disputes involve domestic violence (Chandler, 1990; Keilitz, 1997). In one study, domestic violence offenders were found to be more likely than other fathers to seek custody (Liss and Stahly, 1993). Because of the importance of custody evaluations to the courts and the ultimate outcomes for children and parents, especially in cases of domestic violence (intimate partner abuse), it is critical to have a better understanding of how evaluations are conducted, what factors influence the evaluation, and the extent to which judicial decisions conform to the conclusions and recommendations of the evaluators. In 48 states, courts are required to consider domestic violence in awarding custody and visitation (Family Law Quarterly, Custody Factors Chart, 2009). In some states, as in New York, these statutes require that domestic violence by one parent against the other be considered as a factor in awarding custody; in other states, there is a rebuttable presumption against awarding custody to a parent who has abused the other parent. The appointment and choice of an evaluator may be proposed by the parties or by the attorney for the child or may be chosen by the court without input from the parties or their attorneys. Guidelines or standards for conducting custody evaluations have been issued by professional organizations such as the American Psychological Association (1994, 2009) and the National Council of Juvenile and Family Court Judges (2004, 2006), and government bodies, such as psychology boards (e. Standards for custody evaluators are rarely imposed by the courts: there are typically no requirements for evaluators other than, in some states, professional degrees and licenses (and some states do not even require advanced degrees). Few states require expertise in child development, child abuse, or domestic violence. Assessing and understanding domestic violence as a factor in custody and visitation arrangements requires special expertise. For example, an abuser may appear calm and may be more convincing than a victim, who may appear anxious, depressed, and paranoid. The impact of exposure to domestic violence on the child may be evident in cognitive, social, behavioral, and somatic problems possible responses of which the evaluator should be aware in assessing the child?s best interest. A child may express a preference for the perpetrating parent for a variety of reasons, such as identification with the more powerful parent, a sense that that parent is best equipped to protect the child or has greater ability to provide material benefits, fear of retaliation by the more dangerous parent, or effective manipulation of the child including denigration of the victimized parent. To recognize the different presentations of abusers and victims and the range of reactions of children to exposure to abuse requires specialized knowledge. If an evaluator is assessing the validity of the allegations in order to understand the implications for parenting, the evaluator needs to be aware of the propensity of perpetrators of domestic violence to attempt to control their partners and children, be cognizant of the forms that domestic violence often takes including sexual abuse and patterns of non-physical abuse, including derogation and humiliation, social isolation and financial abuse, and obsessive jealousy expressed in accusations of infidelity used to justify denying the other parent access to the child. Above all, in the assessment of the child?s best interest, evaluators should be aware of the high frequency of child abuse by fathers who abuse their intimate partners. Finally, evaluators who make recommendations to the court about custody and visitation should be aware of the sometimes heightened risk of violence after the couple has separated (American Psychological Association, 2005). Child abuse is frequently a concurrent issue, and common in custody disputes are allegations of parental alienation? claims that one parent has turned the children against the other parent for baseless, vindictive reasons. Ascertaining the validity of accusations of child abuse and parental alienation, and how they should factor into determining the child?s best interest, becomes more complicated in the context of domestic violence and partner abuse. The victim may be naturally fearful of the perpetrating parent and convey that fear to their children, thereby unintentionally distancing the children from the other parent, or the children may be antagonistic to the perpetrating parent because of the abuse they have witnessed. The alleged perpetrator of domestic violence may argue that the claims of abuse are false and intended to alienate the children. On the other hand, domestic violence usually includes denigration of the victim and accusations of inappropriate behavior and children sometimes identify with the perpetrating parent in holding negative views of the victimized parent. These claims and counter claims and the basis of children?s reactions to each parent can be difficult to sort out from the bench. The presence of domestic violence and the frequently co occurring allegations of child abuse may increase judges? reliance on custody evaluators who can observe interactions between parents and children and interview children about what they have seen and heard. Overview and Purpose the primary purpose of this study was to learn about the knowledge and beliefs about domestic violence that custody evaluators bring to their court-ordered task, how they investigate allegations, and how their recommendations relate to court outcomes. To that end, we reviewed case files of legal service attorneys in New York City representing domestic violence victims in custody and visitation proceedings in which the court appointed a custody evaluator. We analyzed and coded the custody evaluators? reports to the court on a large number of dimensions, and compared the evaluators? recommendations to the case outcome (court order or settlement agreement). We also interviewed a subset of the evaluators who wrote the reports in our sample of cases. The definition of domestic violence used by the attorneys who supplied the cases and adopted in the study is intimate partner abuse that constitutes a course of conduct exerting coercive control over the other parent (Stark, 2010; Dalton, Carbon & Oleson, 2003). This definition goes beyond discrete acts of physical assault and incorporates threats and intimidation, social isolation, sexual humiliation, and control and regulation of the partner?s daily life (Stark, 2010). The cases sampled were governed by New York Domestic Relations Law 240 (1)(a), which requires that courts making custody and visitation decisions must consider the effect of such [proven] domestic violence upon the best interests of the child. Did their recommendations for sharing custody between the parents build in protections for the victimized parent? How often did custody evaluators recommend and courts grant custody or unsupervised visitation to alleged abusers? We were also looking for relationships among variables, for example, between the evaluator?s theoretical orientation and knowledge of domestic violence and the evaluator?s recommendations for custody and visitation. We hypothesized that the more knowledgeable the evaluator was about domestic violence, and the more thoroughly the allegations of domestic violence were investigated, the safer the recommended parenting plan would be, in regard to the physical and psychological safety of the victimized parent and the children. We also expected the facts of the case to be influential: we anticipated that the severity of the partner abuse, especially physical abuse, and the better it was documented in the record (e. We hypothesized that there would be a close match between the evaluator?s recommended parenting plan and the parenting plan in the settlement agreement or court order. We thought that the orders crafted by the judge would incorporate more protections for the victimized parent and more restrictions on the noncustodial parent?s visitation than settlement agreements between parents. Our primary expectation was that there would be a great deal of variability in the evaluations, the evaluators? responses to domestic violence allegations, their procedures, and their conclusions. An important concern regarding the appointment of custody evaluators and their influence on the court is that the courts are supposed to provide fair outcomes in accordance with the law. Integral to fairness is consistency in outcomes when the same or similar fact patterns exist. Yet, even when evaluators are conscientious and responsive to the information they gather (including clinical observations), if they have disparate beliefs and levels of knowledge about domestic violence, they are likely to recommend different parenting plans. If some evaluators are not conscientious, or their recommendations are driven by theoretical models of family functioning that promote particular values inconsistent with empirical studies, the results can be devastating for the family. Mothers and fathers who need the court?s intercession in deciding the fate of their children should be able to expect a reasonable outcome that is not dependent on the luck of the draw in the court-appointed evaluator.
Purchase 5mg aygestin fast delivery. Shoufi Mafi : What is your fitness secret? Womens Health Launch.
Some therapists conduct sessions out of the ofce womens health exercise book purchase aygestin 5mg without prescription, by telephone menstruation in the bible purchase aygestin cheap online, online or to fnd people with similar experiences women's health subscription order 5mg aygestin fast delivery. Family members who participate in an individual?s compulsive If Symptoms Return rituals womens health 012013 pl 5mg aygestin sale, provide reassurance or enable avoidance behavior can unintentionally sabotage success in therapy. In some cases, it is helpful for a family member to be trained to act as Obsessive Compulsive Disorder is a chronic condition. Symptoms can be managed, but a coach? to keep track of exposures and discourage behavior by others that perpetuates they sometimes resurface in the same or a diferent form. An individual may not succeed with a particular therapist because the personality ft may not be right, or that therapist may not design Cognitive behavior therapists stress the importance of following through with exposures challenging, appropriate exposures. If this is the case, ask for a second opinion, request or returning symptoms, particularly during stressful times. Booster or refresher therapy a referral or interview other therapists to fnd a good match. A person may enjoy sessions may be necessary from time to time to reinforce treatment gains. Finding a therapist who is right for you is critical to your page) and schedule an appointment. Family members often believe they?re being helpful when they participate in compulsive behaviors. For example, a spouse may agree to sanitize the home, prepare special food, or check and recheck locks. And protecting a family member from the negative consequences of obsessions and compulsions can decrease the motivation for obtaining treatment. For example, a wife who helps her husband with his morning checking compulsions so he won?t be late for work makes it less likely that he?ll seek treatment. It?s important to apply gradual changes, because sudden changes in responses can cause anger and stress that worsen symptoms. Distracting obsessions, time-consuming compulsions, the Social Security and Supplemental Security Income disability programs are the largest avoidance behaviors, and the urge to seek reassurance can prevent an employee or student of several federal programs that provide assistance to individuals with a disability who meet from paying attention and completing work on time. For additional information, call 1-800-368-1019 or visit accommodations or benefts. His mother is now on caring for a child after birth or an employee?s spouse, child, or parent with a serious illness. But some A Complete Guide to Getting Well people fnd that making connections with others who are in the same boat? helps them the Imp of the Mind and Staying Well by Lee Baer, Ph. Non-therapeutic Obsessive-Compulsive Disorder support groups can be extremely benefcial, but they should complement not replace Scrupulosity Demystifed appropriate treatment. Does the group have established ground rules, such as insisting on anonymity and confdentiality? Help for You and Your Family the Secret Lives of Hoarders To Ask Before How often does the group meet, and where? When Perfect Isn?t Good Enough: Do meetings include only open discussion, or are there also programs Strategies for Coping such as flms, lectures, speakers or planned discussion topics? Depending on symptom severity and behavioral, cognitive, and/or environmental factors. In severe cases, people may need to use by resisting the urge to participate in compulsions, reassure or accommodate avoidance medication for longer periods of time. It?s also important for family members to avoid criticizing or nagging, which can cause stress and anger that can make symptoms worse. A: Working with a cognitive behavior therapist, the person creates a list of his or her Q: Is cognitive behavior therapy expensive? Therapy in a group setting is often less expensive than private then avoids performing compulsive behaviors (?response prevention?) for increasingly individual sessions, but it?s important to distinguish between group therapy, which is a longer periods of time. Non-therapeutic groups can be helpful (see page 30), but they are not a replacement for appropriate treatment. Depending on your fnancial situation, you may be able to fnd help through the and their families, and to encourage research into new treatments and a cure. Imagine how much more you?d enjoy every single day if you were free from your obsessions and compulsions. But those who have succeeded in treatment consider the benefts more than worth the efort. Obsessive Compulsive Disorder is a medical problem that requires diagnosis and treatmentObsessive Compulsive Disorder is a medical problem that requires diagnosis and treatment If you found this publication valuable and would like to help bring by a qualifed treatment provider. This guide is not intended to provide, or to take the place of,by a qualifed treatment provider. Any laws or regulations mentioned in this guide are for informational purposes only and doAny laws or regulations mentioned in this guide are for informational purposes only and do not constitute legal advice. For more information about these laws and how they apply to annot constitute legal advice. For more information about these laws and how they apply to an We rely solely on donations from the public. These disorders have enough similarities to group them together in the same diagnostic classification, but enough important differences to exist as distinct subtypes. Information regarding the impact of the subtypes obsessive-compulsive and related disorder due to another medical condition? and substance/medication-induced obsessive-compulsive and related disorder? on youth is limited, so this section will not focus extensively on these subtypes. Compulsions take the form of overt behavioral acts or rituals, or covert mental acts (e. Compulsions may also include repetitive washing, checking, touching, counting, and ordering/arranging. Compulsive hoarding and praying may also occur as a reaction to an obsession (March & Mulle, 1998). Furthermore, children may not be able to specify the consequence of not engaging in their compulsion and may report a vague sense that something bad might happen? if they are not able to complete the compulsion (Barrett et al. Their dependence on their ineffective coping mechanism, in turn, interferes with school, work, and social functioning. The second, substance/medication-induced obsessive compulsive and related disorder, was included because symptoms sometimes develop during or soon after intoxication or withdrawal from a substance or medication. For this diagnosis to be valid, the substance or medication must be capable of causing the symptoms. Individuals with obsessive compulsive disorder now fall into one of the following three categories: good or fair insight, poor insight, or absent insight/delusional. Individuals with good or fair insight understand that their obsessions and compulsions are abnormal or irrational. In contrast, individuals categorized as absent insight/delusional? believe their obsessions and compulsions are normal or rational thoughts, feelings, or actions. This specifier was created to be used as a clinical tool because body dysmorphia varies from other forms of body dysmorphic disorder. There are more problematic risk behaviors associated with body dysmorphia, and evidence suggests treatment methods vary from other forms of body dysmorphic disorder (Phillips, Frost, & Mataix-Cols, 2010). Recurrent and persistent thoughts, urges, or images the youth deems intrusive and unwanted at some point in the experience. Repetitive behaviors or mental acts the youth feels compelled to perform in response to an obsession. Actions are excessive and may not realistically be connected to that which they aim to prevent. The inclusion of this disorder acknowledges that symptoms similar to primary obsessive-compulsive and related disorders can arise as a result of other medical conditions. Symptoms develop during or soon after intoxication or withdrawal from the substance or medication. Data regarding substance/medication-induced obsessive-compulsive and related disorder is Collection of Evidence-based Practices for Children and Virginia Commission on Youth, 2017 Adolescents with Mental Health Treatment Needs 3 Obsessive-Compulsive and Related Disorders extremely limited, but it does indicate that this disorder is very rare. Body dysmorphic disorder causes affected youth to perceive deficits in their physical appearance. However, the body imperfections characterizing body dysmorphic disorder are either not observable or only slightly observable to others. A child or adolescent with body dysmorphic disorder may check the mirror, groom excessively, skin pick, and/or seek reassurance repetitively.
Ranitidine 300 Pantoprazole 40 Pantoprazole 20 Lansoprazole 30 Lansoprazole 15 Esomeprazole 20 0 womens health center 133-03 jamaica avenue discount 5 mg aygestin otc. However women's health center in lebanon pa purchase aygestin with paypal, credible intervals are wide breast cancer t-shirts purchase aygestin 5 mg line, and the data are consistent with most individual options being among the best or among the worst choices pregnancy flu shot buy aygestin discount. The search returned 1864 studies; after title and abstract screening, the full texts of 37 studies were ordered. Therefore, a Markov model with monthly cycles and a lifetime horizon was designed as a simplified representation of the pathway of treatment for people with severe erosive oesophagitis. There are 2 key underlying health states in the model, healed and unhealed oesophagitis, which drive the pathway of treatment. The patient population differs from the focus of this review question as they do not necessarily all have severe reflux oesophagitis. During any model cycle the patient can develop Barrett?s oesophagus, adenocarcinoma or die from other causes. The health states which represent Barrett?s oesophagus and adenocarcinoma capture the health related quality of life and costs of each of the diseases. Anaemia and stricture were identified as complications relevant to unhealed oesophagitis within the modelling framework with associated quality of life values and costs. We assumed that these complications only occur as a result of unhealed oesophagitis; therefore patients in a healed health state cannot develop anaemia and stricture. We configured the models to perform probabilistic sensitivity analysis to quantify uncertainty in the true values of input parameters. Distribution parameters were sourced from the study in which the value was obtained, where possible, or were estimated, based on the usual properties of data of that type. This is not necessarily the same thing as the treatment that has the highest probability of cost effectiveness, as options that are subject to the greatest uncertainty will have a broad spread of results that may include very good and very poor value for money, and it would be a mistake to focus only on probabilities at the positive end of this spectrum. It is because of this kind of variability and asymmetry in the distributions estimated by many health economic models that Fenwick et al. The results presented are for scenarios in which the initial healing/maintenance treatment is reused for any subsequent phases requiring healing/maintenance. An arbitrarily chosen common maintenance treatment is used when the model is configured to provide analysis for the healing and maintenance treatments separately. The treatments which are the most likely to heal the oesophagitis and maintain the healing are also likely to be the most cost-effective treatments. Uncertainty in the estimates of clinical effectiveness manifests itself into uncertainty in the estimates of cost-effectiveness. Increased accuracy in the effectiveness evidence would translate to more confidence in the estimates of cost-effectiveness. Two additional scenarios were tested; 1 in which we assume that after 5 years in a healed state people will not relapse into an unhealed state, and the other in which the initial cohort contains a proportion of patients with Barrett?s oesophagus. The cost-effectiveness results vary slightly but the overriding conclusions are not altered as a result. An additional scenario was explored in which a direct relationship between healing and symptoms was estimated. This generated a paradoxical incentive to fail treatment and for progress to be managed by a specialist, because this would result in a faster resolution of symptoms and thus improvement to quality of life. Additional information on the modelling methods and parameters used as well as a discussion of the results is provided in appendix H. An original economic model with Markov health states showed that the treatments that are most likely to be clinically effective in the healing of severe oesophagitis are also the most likely to be cost-effective. An original economic model with Markov health states, showed that the treatments that are most likely to be clinically effective in the maintaining of the healing of severe oesophagitis are also the most likely to be cost-effective. All the included studies had 6 to 12 months? follow-up, which did not reflect the real clinical picture that most people with severe erosive reflux disease are likely to be on life-long treatment. The model hinged on 2 key health states healed and unhealed oesophagitis which determine the sequence of treatment offered and the probability of developing complications such as anaemia, stricture, Barrett?s oesophagus and adenocarcinoma (oesophageal or gastric). Healing phase the economic model suggested that the most effective treatments are likely to be the most cost-effective options. Maintenance phase (prevention of relapse) Evidence was available for only 5 maintenance regimens, and this reduced the options that could be considered in the economic model. A systematic search was conducted (see appendix C) which identified 2398 references. After removing duplicates the references were screened on their titles and abstracts and 142 references were requested (6 papers were unavailable) and reviewed against the inclusion and exclusion criteria (appendix C). Overall, 105 studies were excluded as they did not meet the eligibility criteria because of study design or relevant controls or interventions. An update search had also identified an additional study that met the inclusion criteria. Data was extracted into detailed evidence tables (see appendix D) and are summarised in Table 36 below. The overall quality of the 32 (31 from the original search with 1 additional from the update search) included studies was of poor/very poor quality with low and very low confidence in the effect estimates. Thirteen out of the 31 included studies were retrospective studies and the majority of the included studies were case control studies, with a small number of cross sectional studies (prevalence studies). Issues on study design There were a number of methodological issues of the included studies that might contribute to substantial risk of bias, for example:? There were different definitions used for confirming Barrett?s oesophagus (histological or biopsy or both) among the included studies. Only 1 study (Thrift, 2012) had carried out validation study of the prediction model to another population. Hence, the utility of these risk factors were questionable as the purpose of the evidence review was to provide guidance on who and with which National Institute for Health and Care Excellence, 2014. Nevertheless, the evidence on these risk factors was synthesised for completeness of the evidence-base. Issues on statistical analysis As well as issues on study design, the included studies also suffered a number of limitations on statistical analysis. All included studies used multivariate analyses (logistic regression) to analyse collected data. However, different predictive variables (risk factors) were included in different studies in the regression models. For example (key diagnostics): o Assumptions of normality and homoscedasticity were not tested. Due to all the above methodological and statistical issues, meta-analyses on individual risk factors were not appropriate. Where appropriate, the evidence is presented by outcome (risk factors) even though meta-analysis was not possible. However, where there was only 1 included study on certain subgroups or specific predicted endpoint, the evidence is presented by individual study. Age: 61 years (mean) Symptoms, Ulcer, significant predictors of Eight sites multicentre study. No model diagnostics but the Case control Barrett?s oesophagus defined as: Presence of model was controlled for age, 112 Dyspepsia and gastro-oesophageal reflux disease study intestinal metaplasia with goblet cells on biopsy gender and centre as potential sample confounders. Barrett?s oesophagus defined as: Histology with No model diagnostics and no Cross presence of intestinal metaplasia with goblet control for potential confounders. Symptoms, Duration, Regurgitation, questionnaire were more likely to Gender: Male 96% Medication Frequency of be African American (p<0. No model diagnostics but the Barrett?s oesophagus defined as: Goblet or model was controlled for potential Case control confounders. Two sites cross biopsy confirmation fo intestinal metaplasia, the multicentre study. Retrospectiv e Age: Mean age not reported observationa Barrett?s oesophagus defined as: Intestinal l cohort metaplasia was defined as presence of goblet 114 Dyspepsia and gastro-oesophageal reflux disease study cells on biopsy. No central verification of histo pathological or endoscopic findings was possible. Cross Barrett?s oesophagus defined as: Segments of sectional intestinal metaplasia on biopsy. No items from Barrett?s oesophagus defined as: presence of symptom questionnaire were Prospective intestinal metaplasia on biopsy of salmon significant in multivariate cohort study coloured mucosa regression analysis.