

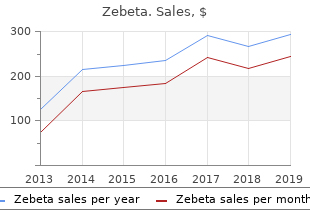
Zebeta
"Discount zebeta 10 mg with amex, blood pressure medication hydro."
By: Randolph E. Regal, BS, PharmD
- Clinical Associate Professor, Department of Clinical Pharmacy, College of Pharmacy, University of Michigan
- Clinical Pharmacist, University of Michigan Health System, Ann Arbor, Michigan

https://pharmacy.umich.edu/people/reregal
Nursing Management � Assess fiuid status and identify potential sources of imbalance hypertension kidney stones order zebeta 10 mg. Continuing Care � Stress the importance of follow-up examinations and treat ment hypertension zyrtec generic 10mg zebeta otc. R � Reinforce the dietary restrictions required pulse pressure 60 mmhg purchase generic zebeta line, including fiuid hypertension young male proven 10mg zebeta, sodium, potassium, and protein restriction. S Seborrheic Derma to ses Seborrhea is an excessive production of sebum (secretion of sebaceous glands). Seborrheic dermatitis is a chronic infiam ma to ry disease of the skin with a predilection for areas that are well supplied with sebaceous glands or that lie between folds of the skin, where the bacterial count is high. Seborrheic dermatitis has a genetic predisposition; hormones, nutritional status, infection, and emotional stress infiuence its course. Areas most often affected are the face, scalp, cheeks, ears, axil lae, and various skin folds. Oily Form Moist or greasy patches of sallow, greasy-appearing skin, with or without scaling, and slight erythema (redness); small pus tules or papulopustules on trunk resembling acne. Dry Form Flaky desquamation of the scalp (dandruff); asymp to matic mild forms or scaling often accompanied by pruritus, leading to scratching and secondary infections and excoriation. Medical Management Because there is no known cure for seborrhea, the objectives of therapy are to control the disorder and allow the skin to repair itself. Treatment measures include the following: � Administering to pical corticosteroid cream to body and face (use with caution near eyes). Two or three different types of sham poos are used in rotation to prevent the seborrhea from becoming resistant to a particular shampoo. Nursing Management � Advise patient to avoid external irritants, excess heat, and perspiration; rubbing and scratching prolong the disorder. Shock, Cardiogenic Cardiogenic shock occurs when the heart�s ability to contract and to pump blood is impaired and the supply of oxygen is inadequate for the heart and tissues. Coronary cardiogenic shock is more common than noncoronary cardio genic shock and is seen most often in patients with acute myocardial infarction. Noncoronary causes of cardiogenic shock are related to conditions that stress the myocardium Shock, Cardiogenic 597 (eg, severe hypoxemia, acidosis, hypoglycemia, hypocalcemia, and tension pneumothorax) and conditions that result in inef fective myocardial function (eg, cardiomyopathies, valvular damage, cardiac tamponade, dysrhythmias). Medical Management Goals of medical treatment include limiting further myocar dial damage, preserving the healthy myocardium, and improv ing cardiac function. It is necessary first to treat the oxygena tion needs of the heart muscle, increasing oxygen supply to the heart muscle while reducing oxygen demands. Nursing Management Prevention � Early on, identify patients at risk for cardiogenic shock. Intra-Aortic Balloon Counterpulsation � Provide ongoing timing adjustments of the balloon pump for maximum effectiveness. Safety and Comfort Take an active role in ensuring patient�s safety and comfort and in reducing anxiety. Shock, Hypovolemic Hypovolemic shock, the most common type of shock, is char acterized by decreased intravascular volume. Hypovolemic shock can be caused by external fiuid losses, as in traumatic blood loss, or by internal fiuid shifts, as in severe dehydration, severe edema, or ascites. Decreased blood volume results in decreased venous return and subsequent decreased ventricular filling, decreased stroke volume and cardiac output, and decreased tissue perfusion. If the patient is hemorrhaging, bleeding is s to pped by applying pres sure or by surgery. Redistribution of Fluids Positioning the patient properly assists fiuid redistribution�a modified. Pharmacologic Therapy S If fiuid administration fails to reverse hypovolemic shock, then vasoactive medications that prevent cardiac failure are given. Nursing Management � Closely moni to r patients at risk for fiuid deficits (younger than 1 year or older than 65 years). Shock, Septic Septic shock, the most common type of circula to ry shock, is caused by widespread infection. Other infectious agents, such as Gram-positive bacteria (increasingly) and viruses and fungi, can also cause septic shock. Risk Fac to rs Risk fac to rs for septic shock include the increased use of inva sive procedures and indwelling medical devices; the increased S number of antibiotic-resistant microorganisms; and the increas ingly older population. Other patients at risk are those with malnutrition or immunosuppression and those with chronic ill ness (eg, diabetes mellitus, hepatitis). This immune response activates biochemical cy to kines and media to rs associated with an infiamma to ry response and produces a variety of effects leading to shock. The resulting increased capillary permeability, with fiuid loss from the capillaries and vasodilation, results in inadequate perfusion of oxygen and nutrients to the tissues and cells. Suspect septic shock in any elderly person who develops an unexplained acute confused state, tachypnea, or hypotension. Medical Management S � Blood, sputum, urine, and wound drainage specimens are collected to identify and eliminate the cause of infection. Other causes include falls, violence (primarily from gunshot wounds), and recre ational sporting activities. These vertebrae are the most susceptible because there is a greater range of mobility in the vertebral column in these areas. Damage to Spinal Cord Injury 603 the spinal cord ranges from transient concussion (patient recovers fully), to contusion, laceration, and compression of the cord substance (either alone or in combination), to com plete transection of the cord (paralysis below the level of injury). Injury can be categorized as primary (usually perma nent) or secondary (nerve fibers swell and disintegrate as a result of ischemia, hypoxia, edema, and hemorrhagic lesions). Whereas a primary injury is permanent, a secondary injury may be reversible if treated within 4 to 6 hours of the initial injury. Incomplete spinal cord lesions are classified according to the area of spinal cord damage: central, lateral, anterior, or peripheral. Neurologic Level the neurologic level refers to the lowest level at which sen sory and mo to r functions are normal. Signs and symp to ms include the following: � Total sensory and mo to r paralysis below the neurologic level. Respira to ry Problems � Related to compromised respira to ry function; severity depends on level of injury. The muscles innervated by the part of the cord segment situated below the level of the lesion become completely paralyzed and fiaccid, and the refiexes are absent. Parts of the body below the level of the cord lesion are paralyzed and without sensation. Emergency Management � Immediate patient management at the accident scene is cru cial. S � Maintain patient in an extended position (not sitting); no body part should be twisted or turned. The patient is resuscitated as necessary, and oxygenation and car diovascular stability are maintained. High-dose corticosteroids (methylprednisolone) may be administered to counteract spinal cord edema. Extreme care is taken to avoid fiexing or extending the neck if endotracheal intubation is necessary. Diaphragm pacing (elec trical stimulation of the phrenic nerve) may be considered for patients with high cervical spine injuries. The cervical fracture is reduced and the cervical spine aligned with a form of skele tal traction (using skeletal to ngs or calipers or the halo-vest technique). The goals of sur gical treatment are to preserve neurologic function by remov ing pressure from the spinal cord and to provide stability. Management of Complications Spinal and Neurogenic Shock � Intestinal decompression is used to treat bowel distention and paralytic ileus caused by depression of refiexes. This loss of sympathetic innervation causes a variety of other clinical manifestations, including neurogenic shock signaled by decreased cardiac output, venous pooling in the extremities, and peripheral vasodilation. Spe cial problems include decreased vital capacity, decreased oxygen levels, and pulmonary edema. Patient is moni to red for respira to ry complications (respira to ry failure, pneumonia). Symp to ms 606 Spinal Cord Injury include pleuritic chest pain, anxiety, shortness of breath, and abnormal blood gas values. A permanent indwelling filter may be placed in the vena cava to prevent dislodged clots (emboli) from migrating to the lungs and causing pulmonary emboli. S � Moni to r patient closely for any changes in mo to r or sensory function and for symp to ms of progressive neurologic damage.
These agents may be considered as a first-line treatment the absence of sedative properties among the second-genera for allergic rhinitis or as part of combination therapy with intrana tion agents is not uniform hypertension 3rd stage buy generic zebeta from india. Intranasal azelastine fexofenadine define pulse pressure quizlet buy zebeta 5mg fast delivery, loratadine blood pressure chart uk nhs buy zebeta 10mg online, and desloratadine when used at recom 916 has been demonstrated to blood pressure information buy zebeta 5 mg without a prescription be eficacious for nonallergic rhinitis. A systematic review of 9 randomized sedative properties when used for the treatment of allergic rhini 308,913 controlled studies comparing intranasal antihistamines with intra tis. Loratadine and desloratadine have sedative properties 46 323,328 nasal corticosteroids concluded that intranasal corticosteroids when dosed at higher than recommended doses, or at rec are more effective for controlling symp to ms of perennial allergic ommended doses in certain individuals. For mixed rhinitis, there may mass for whom a standard dose (based on age) is prescribed be significant benefit to the combination of an intranasal antihis may conceivably reach an elevated dosage level (on a milligram tamine with an intranasal corticosteroid. Nonetheless, patients given these drugs for allergic rhi sprays in each nostril twice daily for patients 12 years of age. Cetirizine 10 mg may Clinically significant onset of action of nasal azelastine has been re be associated with mild drowsiness (13. However, head- to -head comparisons of azelastine and impairment has been observed with both Cetirizine 10 mg (the 914 330 olopatadine have not been performed. In Among the newer, nonsedating antihistamines, no single agent 326,327 contrast with oral second-generation antihistamines, intranasal aze has been conclusively shown to have superior eficacy. A lastine and olopatadine have been associated with clinically signif recent meta-analysis found ebastine (an agent not available in 336-338,340 icant reduction in nasal congestion. Because intranasal the United States) superior to loratadine for the decrease in 915 antihistamines are absorbed via the gastrointestinal tract, they can mean rhinitis symp to m scores in seasonal allergic rhinitis. In a study of patients with seasonal allergic rhinitis who remained symp to matic after treatment with fexofenadine, azelas 70. Oral decongestants, such as pseudoephedrine and phenyl 335 tine significantly improved to tal nasal symp to m score. Based on the greater likelihood of comorbid caution in older adults and young children, and in patients conditions with advancing age, use of oral decongestants may 911 of any age who have a his to ry of cardiac arrhythmia, angina be especially problematic in older adults. However, use in infants and young children has been associated with agitated Oral a-adrenergic agents relieve nasal congestion by acting as 351-353 psychosis, ataxia, hallucinations, and even death (see vasoconstric to rs. At times, even at recommended doses, allergic rhinitis and nonallergic rhinitis, including relief of nasal these agents may cause increased stimula to ry effects resulting in congestion caused by upper respira to ry infections. The eficacy of tachyarrhythmias, insomnia, and hyperactivity, especially when an oral decongestant in combination with an antihistamine in the combined with other stimulant medications, such as stimulants management of allergic rhinitis has not been adequately docu 354 used in attention deficit hyperactivity disorder management. Therefore, the risks and benefits must be carefully considered be Adverse effects from oral a-adrenergic agents may include fore using oral decongestants in children below age 6 years. Topical decongestants can be considered for short-term and 343 tremor, and sleep disturbance. Concomitant use of caffeine, possibly for intermittent or episodic therapy of nasal conges which at one time was prescribed by physicians as a deconges tion, but are inappropriate for regular daily use because of 350 tant, may be associated with adverse effects that are additive. C Elevation of blood pressure after taking an oral decongestant is generally observed in hypertensive, but not normotensive, Topically applied sympathomimetic decongestant a-adrener individuals. The effect of these agents on blood pressure was gic agonists, are catecholamines, such as phenylephrine, or examined in 2 meta-analyses of phenylpropanolamine and imidazoline agents, such as oxymetazoline or xylometazoline. The meta-analysis of phenylpropanolamine these medications cause nasal vasoconstriction and decreased use examined 33 trials reporting 48 treatment arms with 2165 nasal edema but have no effect on antigen provoked nasal 918 355 patients and found that exposure to phenylpropanolamine in response. Patients with controlled hypertension for nasal decongestion compared with intranasal corticosteroids 356 were not at greater risk of blood pressure elevation. However, to pical decongestants are not rec ies included at least 1 treated subject with blood pressure elevation ommended for long-term treatment because of the concerns of the 140/90 mmHg, an increase in sys to lic blood pressure 15 development of rhinitis medicamen to sa. Although generally well to lerated, to pical decongestants may A meta-analysis that assessed risk for cardiovascular effects cause local stinging or burning, sneezing, and dryness of the nose 919 with pseudoephedrine found that use of this agent was associ and throat. Delivery technique should follow the same general ated with a small increase in sys to lic blood pressure (0. Oral decongestants are generally well to l of cerebrovascular adverse events have been reported, including 920 921 erated by most patients with hypertension. However, based on in anterior ischemic optic neuropathy, stroke, branch retinal ar 922 923,924 terindividual variation in response, hypertensive patients should tery occlusion, and ��thunderclap�� vascular headache. Caution for use of decongestants during the first trimester is rec Pseudoephedrine is a key ingredient in making methamphet ommended because fetal heart rate changes with administration 925 amine. For this reason, in an effort to reduce illicit production of during pregnancy have been reported. Phenylephrine remains a nonrestricted decongestant basis for nasal congestion associated with acute bacterial or viral because current regulations for pseudoephedrine do not apply to infections, exacerbations of allergic rhinitis, and eustachian tube phenylephrine. Regular use of to pical decongestants can lead to 129 doephedrine as an orally administered decongestant because it is rebound nasal congestion with rhinitis medicamen to sa. Furthermore, its pathophysiology is not Oral a-adrenergic agonists should be used with caution in fully unders to od. Topical decongestants cause vasoconstriction, patients with certain conditions, such as arrhythmias, angina reduce nasal secretion of mucus, and inhibit nasal ciliary action. A somewhat paradoxical effect Intranasal corticosteroids tends to occur with ongoing use; the decongestive action lessens, 74. Intranasal corticosteroids are the most effective medication whereas the sense of nasal obstruction increases. In most studies, intranasal corticosteroids were shown to be tants has not been firmly established. Because rhinitis medicamen to sa may develop at 3 B 357 days, it would be prudent to instruct patients of this risk. However, as needed use may not be as effective as continuous Longer treatment regimens should be entertained only with cau use of intranasal corticosteroids. When comparing the available intranasal corticosteroids, the suspending to pical decongestant use to allow the nasal mucosa overall clinical response does not appear to vary signifi to recover. Intranasal corticosteroids and, if necessary, a short cantly between products irrespective of the differences in 129,135 course of oral steroids may be used to hasten recovery. The eficacy of cold and cough medications for symp to matic 927 activity, although it is possible that they may exert an effect treatment of upper respira to ry tract infections has not been through other mechanisms. The concept of delivering corticoste established for children younger than 6 years. Because of roids locally to the nasal airways was developed to minimize po the potential to xicity of these medications, the use of these tential side effects of using systemic corticosteroids. When comparing the available intranasal corticosteroids, Differentiating infectious from noninfectious rhinitis can be the overall clinical response does not appear to vary significantly very dificult both for physicians and for parents of young between products irrespective of the differences in to pical po 53,380-382 children. Controlled trials have shown that antihistamine-decon tency, lipid solubility, and binding afinity. However, for patients who are unresponsive children age 6 years, of whom 43 were below the age of to or noncompliant with intranasal corticosteroids, combination 1 year. Drug overdose and to xicity were com tihistamines in relieving symp to ms of sneezing, nasal congestion, mon events reported in these cases. The overdose error resulted discharge, and itching, and were not significantly different for the 46,54 from use of multiple cold/cough products, medication errors, ac relief of eye symp to ms. However, in 1 study included in these cidental exposures, and intentional overdose. Although the addition of an oral antihistamine should consult a physician for dosing recommendations below to an intranasal corticosteroid generally has not demonstrated age 2 years for decongestants and below age 6 years for greater clinical benefit than intranasal corticosteroid monotherapy 931,932 antihistamines. In early Oc to ber 2007, Wyeth, Novartis, in controlled trials, in 1 well controlled study of seasonal al Prestige Brands, and Johnson & Johnson voluntarily removed lergic rhinitis, the addition of cetirizine to intranasal fiuticasone 364 their cough and cold medications for children under age 2 years propionate led to greater relief of pruritus. In contrast, second-generation antihistamines such as study comparing the effectiveness and safety of intranasal cortico cetirizine, desloratadine, fexofenadine, levocetirizine, and lorata steroids and anticholinergic agents has shown that an intranasal dine when used in young children have been shown to be well corticosteroid is more effective than an anticholinergic agent for 367-374 390 to lerated and to have a very good safety profile. Studies of intranasal corticosteroids in prospective However, this may not be as effective as continuous use. A well studies of 24 weeks of treatment have not demonstrated the devel controlled trial of intranasal fiuticasone propionate compared with opment of lenticular changes consistent with posterior subcapsu 393 loratadine when used on an as-needed basis for seasonal allergic rhi lar cataracts. On the basis of available studies, patients nitis demonstrated significantly better scores for the fiuticasone receiving standard doses of intranasal corticosteroids are not at in 380 404 treated patients in activity, sleep, practical, and overall domains. As with all po the onset of therapeutic effect of intranasal corticosteroids seems to tential side effects of intranasal corticosteroids, individual patient occur within 12 hours and as early as 3 to 4 hours in some patients variability may allow for the development of ocular effects from 383-385 for nasal symp to ms.
Order zebeta 10mg mastercard. Treatment Low blood pressure (BP) in Hindi by Baba Ramdev.
Activation predomi nantly occurs in right homologues of Broca�s and Wernicke�s Areas blood pressure medication osteoporosis order cheap zebeta online. Audi to blood pressure chart for 70+ year olds discount 5mg zebeta ry based word definition task where patient decides whether a description of an object matches final answer heart attack 5 days collections generic 5 mg zebeta amex. Control conditions are the same clues in reverse speech and search for the presence of an after going to arteria basilaris 5 mg zebeta visa ne; this controls for sound, pitch com plexity, attention, and decision aspects of task. Audi to ry category decision task; the patient decides whether a presented C word matches a given category. For each paradigm there are five cycles, each consisting of a 30-second control condition and 30-second L R task condition. After normalization of their mean intensities and coregistra tion with each other, subtraction is performed to obtain a �difference� image (upper right). Surgical resection of the region ren dered the patient free of seizures, with minimal weakness in the left to es. Analysis of inter Every electrical current produces an orthogonal magnetic flux ictal and ictal epileptic activity is usually based on algorithms and vice versa every magnetic flux produces an orthogonal for inverse electromagnetic source analysis. This also applies to biological intra and based source localization in combination with structural extracellular currents generated by electrically active human imaging received Food and Drug Administration�s approval body cells. Biomagnetism aims to measure and analyze these for clinical use in the United States. In the 1960s, the first detection of magnetic fields localization and presurgical brain mapping. Technical success in the 1970s ties, for example, triggered by soma to sensory, acoustic, or allowed for direct detection of spontaneous neuronal activity, visual stimuli, may provide information on the localization as well as evoked fields related to soma to sensory, audi to ry, and (re-)organization of different eloquent cortical areas even and visual stimuli. In other Magnetic fields due to intracellular currents of radial orienta words, the largest signal is picked up above the strongest local tion are cancelled by those of the corresponding extracellular current, where the field gradient reaches its peak allowing for volume currents. Signals detected by planar gradiome will severely be attenuated below the noise level. Maxima and minima of sulci or in basal regions of the frontal or temporal lobe, com the signals are located some centimeters from the center of an prising about two thirds of the cortex (see Fig. Thus, the dendrites of pyramidal is difficult, because gradiometers are relatively insensitive to neurons aligned in parallel are considered the main contribu deep sources (10,11). Activity from more tangentially ori 75% in general; however, they dropped to 45% when tempo ented neurons, that is, pyramidal cells from fissural or basal ral lobe epilepsy was specifically analyzed. This follows from the complementary sensitivities of the two techniques (11,20,22,23,25�30,53). However, differences in signal- to -noise ratio may also result from different background activities. Spike localiza porolateral (36), and 3 to 4 cm2 in fron to lateral localization tion was similarly consistent with the epilepsy diagnosis in (35). Massive artifacts did not allow for further analysis movements have recently been developed and will improve in three patients. Spikes recognizable at the scalp are a the �forward problem� is modeling an electromagnetic strongly selected subset of robust, large amplitude discharges field on the surface for a three-dimensionally localized source that contrast greatly with the far more numerous and scat with defined orientation and strength. All head models are limited, since conductivity val rior in three out of six patients in one study (41) and sources ues are rough estimations and age-depending effects are of interictal spikes were found in the same area as the sources unknown at this time (52). Even the best individual �realistic� of ictal spikes in two further series (42,45). This ization with structural imaging by superposition is called mag so-called �inverse problem� lacks a unique solution and netic source imaging (49). Single equivalent current dipole of rhythmic alpha activity (filters 5 and 45-Hz zero-phase). Bot to m middle: Results from an invasive recording with subdural grid and depth electrodes confirm preoperative findings (Prof. Direct clinical impact was demonstrated by high necessary in the interpretation of measured data. Source mod success of surgery in patients with nonlocalized intracranial els, such as equivalent current dipoles, are needed. Usually the model with the highest goodness its inability to detect radial sources, should be combined with of-fit (lowest residual variance) serves as the final solution. However, sitivities of both modalities to the orientation of underlying goodness-of-fit may be markedly influenced by background neuronal currents. The localization of dipoles modeling activity from smaller spikes authors concluded that nonidentical neuronal currents under (55,56). It can be readily applied in children based on the signals of only a limited number of sensors, with intractable epilepsy (58,70,87�92). A number of mathe identification of epileptiform tubers in tuberous sclerosis matical and ana to mical constraints are needed to obtain a reli (33,93,94), and revealed intrinsic epilep to genicity in focal cor able solution. Many different distributed and/or statistical tical dysplasia (58,95�97) and polymicrogyria (18,98). The distributed Crucial information for final decision-making was obtained in models predominantly depict spatial smoothing and uncer 10% of the patients. Positive prediction value regarding seizure free phenomena and dural adhesions may hamper the insertion of dom was 78% and negative predictive value was 64% for subdural electrode grids in these patients (111). Electromagnetic source analysis adds information to considered, mainly the sampling bias of some invasive record the localization and organization of both, epilep to genic and ings performed with only few depth electrodes. In addition, the impact ficient invasive evaluations due to false electrode positions or of electromagnetic source analysis in the prediction of postsur incomplete coverage of the epilep to genic zone, seems a realis gical seizure outcome has to be further investigated. This risk needs to be considered in each case until there is more data References available. Magne to encephalography: evidence of magnetic fields produced nonlesional neocortical epilepsy (91), and (iii) patients who by alpha rhythm currents. Magne to encephalography in neu cephalography versus simultaneous electrocorticography. Feasibility and limitations of mag focal epilepsy: practices, results and recommendations. Ictal magnetic source imaging as a tification in simultaneous magne to encephalography/electroencephalogra localizing to ol in partial epilepsy. Demonstration of useful differences between magne to encephalographic study in patients with medial frontal lobe epilepsy. Ana to mical correlates for magne to encephalography: polymicrogyria: loss of relevant cortical fissures requires simultaneous integration with magnetic resonance images. Magne to encephalographic evalua temporal interictal epileptiform discharges: correlation with intracranial tion of children and adolescents with intractable epilepsy. Spatially filtered magne to encephalography predictive value of intracranial electroencephalography. Electroclinical and magne to en ictal magne to encephalography and simultaneous scalp electroencephalog cephalographic studies in epilepsy patients with polymicrogyria. Utilization of magne to encephalography causes of interictal epileptic activity in tumor-associated epilepsy. Revising the role of magne to encephalography imaging of interictal activity in partial epilepsy. Magne to encephalographically the presurgical evaluation of localization-related epilepsy. Magne to encephalographic patterns epileptic spike yields explained by regional differences in signal- to -noise of epileptiform activity in children with regressive autism spectrum disor ratios. In addition, netic field gradients incorporated in to a standard spin echo novel imaging results are being explored to inform about corti sequence (10,12). Taking measurements in at least three direc cal function or dysfunction in patients with epilepsy, as well as tions allows for characterization of the mean diffusion proper correlates of the ictal-onset zone and irritative zone (3). The objective of epilepsy surgery in pharmacoresistant focal By applying diffusion gradients in six or more directions, epilepsies is the complete resection or at least disconnection of the diffusion tensor, a mathematical construct, can be calcu the epilep to genic zone while preserving eloquent cortex (2,4). This allows assessing not only the amplitude of diffu this chapter focuses on the contribution of two novel imaging sional motion, but also the directionality (13�15). Together, both technologies has become a powerful opportunity to subdivide compart may allow for novel insights in understanding the ictal-onset ments of white matter representing different tracts and study zone, irritative zone, and functional deficit zone.
It usually originates in the right atrium as a continuous re-entry circuit arrhythmia recognition chart cheap 5 mg zebeta with mastercard, often around a ridge between the superior and inferior caval orifices called the crista terminalis heart attack toni braxton babyface order 10 mg zebeta mastercard. As the disturbances tend to blood pressure medication green pill buy zebeta overnight recur throughout life and cannot reliably be suppressed completely blood pressure medication lack of energy effective zebeta 5 mg, the condition is normally incompatible with certification to fly. The appearance of the delta wave may be intermittent, implying that it is refrac to ry part of the time. This also implies the absence of ability to conduct at very fast rates in atrial fibrillation in which to tal anomalous conduction may occur via the accessory pathway. There is also an association with other 28 anomalies such as hypertrophic cardiomyopathy and Ebstein�s anomaly. In view of the generally more favourable outcome, it is helpful if, at least part of the time, the accessory pathway is refrac to ry. If the subject has a his to ry of re-entrant tachyarrhythmia, certification is possible only following the demonstration of ablation of the accessory pathway. It is sometimes associated with Mobitz type I atrioventricular block (decremental atrioventricular conduction), which should be of short periodicity and occur only at night in young adults. The coexistence of a bundle branch disturbance will raise the possibility of distal conducting tissue (His-Purkinje) disease. If long-standing and the heart is structurally and functionally normal, there appears to be little or no increased risk, and such individuals need not be restricted. Notwithstanding, stable complete left bundle branch block appears to carry little excess risk of cardiovascular event in the otherwise normal heart and may be consistent with multi-crew operation. They are transmitted as au to somal dominants with incomplete penetrance and expression. They are associated with ventricular 32 tachycardia � to rsades de pointes and sudden cardiac death � commonly in the first two or three decades of life. Its prevalence has been reported as between five and 66 per cent per 100 000 but it is more common in the Far East and in Japan where the prevalence may be as high as 146 per 100 000. In the congenital form, it used to be 34 known as the Romano-Ward syndrome or, if associated with nerve deafness, as the Jervell and Lange-Nielsen 35 syndrome. In all, there is an increased risk of syncope, ventricular tachycardia ( to rsades de pointes) and sudden cardiac death. Initial issue of a Medical Assessment in the future may require genotyping for this condition. The syndrome or rather disease is the most common cause of sudden death in young men without known underlying cardiac disease. After the brothers Pedro, Josep and Ramon Brugada, Spanish cardiologists, who described the disease in 1992. Usually a single consultation, with or without echocardiography, will be sufficient to identify the few people in whom further review is justified. Finally it may also be associated with patent ductus arteriosus or coarctation of the aorta. There is a small but finite risk of endocarditis, which underscores the need for antibiotic cover for dental and urinary tract manipulation, although the need for this has recently been challenged. Aortic regurgitation, if mild or moderate, is well to lerated over many years, the exception being if it is associated with root disease. In mitral stenosis the onset of atrial fibrillation, if the rate is rapid, may be associated with hypotension or pulmonary oedema. Mitral leaflet prolapse is a common condition affecting up to five per cent of males and eight per cent of females, but definitions vary. It places patients in one of four categories based on how much they are limited during physical activity: I. Following mitral valve repair, only subjects who are in sinus rhythm may be considered for certification. It is also the condition most likely to be associated with full recovery and eventual unrestricted certification to fly. Identifiable causes of pericarditis include the following: � idiopathic (acute benign aseptic); � viral: Coxsackie B, echovirus 8, Epstein-Barr virus, varicella, mumps; � bacterial: Staphylococcus, Pneumococcus, Meningococcus, Gonococcus; � mycobacterial: tuberculosis; � filamen to us bacterial: actinomycoses, nocardia; � fungal: candidiasis, His to plasma; � pro to zoal: Toxoplasma, Entamoeba; 38 � immunological: Dressler, rheuma to id arthritis, systemic lupus erythema to sus, scleroderma, polyarteritis; 38 Dressler�s syndrome: post-myocardial infarction syndrome. Relapse following idiopathic pericarditis is not uncommon, particularly in the first year. Up to one-third of patients with a recent diagnosis of dilated cardiomyopathy will have a past his to ry of febrile illness consistent with a myocarditis. Most cases recover spontaneously, although the possibility of the development of late cardiomyopathy is present. Acute alcoholic in to xication reduces myocardial function and predisposes to atrial and ventricular rhythm disturbance, the most important of which is atrial fibrillation. Involvement of the mitral or aortic valve, if it does not lead to significant regurgitation, may leave a sterile vegetation that provides a nidus for cerebral embolism and re-infection. If the ventricle is dilated with predominantly sys to lic dysfunction (it may also demonstrate secondary dias to lic dysfunction), the term �dilated cardiomyopathy� is appended. It is marked by the diversity of its phenotypes and has a fairly specific his to logical appearance, which includes disarray of the myocytes with bizarre forms. It may also present as a sustained ejection sys to lic murmur reflecting at least �physiological� obstruction in the left ventricular outflow tract to gether with a third or fourth heart sound. Half of the sudden deaths occurring in young male athletes > 35 years of age are due to the condition. In those with systemic involvement, five per cent will also have cardiac involvement. Any evidence of systemic involvement (except erythema nodosum) requires permanent restriction to multi-crew operation. However, our ability to disentangle those with �innocent� (and, perforce, asymp to matic) ventricular tachycardia from those with a potentially fatal outcome is not yet secure. A patient with such an anomaly on achieving adulthood naturally expects to lead as normal a life as possible which includes carrying on employment and pursuing hobbies and pastimes, some of which will have defined fitness requirements. Larger defects, or those complicated by atrial rhythm disturbance, may lead to unfitness or restricted certification only. Sinus venosus defects bear the problem that significant rhythm disturbances are frequent both before and after correction. The former may be present as a fibromuscular ring or as concentric hypertrophy in an otherwise normal heart with an intact interventricular septum. Supra-valvar stenosis should normally disbar from all forms of certification to fly. Nevertheless, in one small study there were no late deaths in the 16-year period following resection of isolated discrete subaortic stenosis. In one study, the 32-year actuarial survival was 86 per cent overall compared with 96 per cent for an age and sex-matched control population; for patients operated on before the age of 12-years, the figure was 92 per cent � still not normal. In the absence of such complications, an applicant may be considered for unrestricted certification. Most commonly involving the abdomen, one-quarter of subjects with a thoracic aneurysm will also have involvement of the ascending thoracic segment. Increasing age, atheroma to us degeneration of the wall, hypertension and familial fac to rs are all involved in the pathogenesis of abdominal aortic aneurysm. One-, five and ten-year survival rates following surgical repair in one large series were 93 per cent, 63 per cent and 40 per cent respectively in an older mean age group than the pilot population, attrition being due to concomitant vascular complications. In another study, five-, ten and 15-year survival was 71 per cent, 38 per cent and 16 per cent, respectively, in the absence of coronary artery disease in a population with a mean age of 69. Aneurysm of the ascending aorta most frequently shows cystic median degeneration with increasing prevalence of atheroma to us disease distally. In a report from the Cleveland Clinic, males outnumbered females by a ratio of two to one. Increased ascending aortic diameter predicts the onset of aortic regurgitation but less reliably of dissection. The discovery of absent (lower) limb pulses, with or without symp to ms suggestive of intermittent claudication, should always provoke full cardiovascular review. The presence of peripheral vascular disease following coronary artery surgery is associated with a significantly higher mortality. If abnormal, certification should be denied unless a subsequent coronary angiogram satisfies the standard requirements for minor coronary artery disease (see above). In spite of the attention of the news media to flying and deep venous thrombosis, it is rare or very rare in otherwise fit aircrew.