

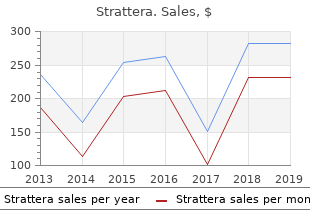
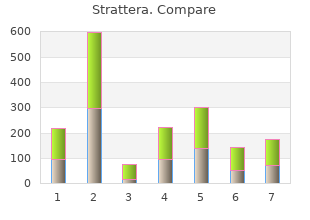
Strattera
"Discount 40mg strattera with visa, treatment qt prolongation."
By: Denise H. Rhoney, PharmD, FCCP, FCCM
- Ron and Nancy McFarlane Distinguished Professor and Chair, Division of Practice Advancement and Clinical Education, UNC Eshelman School of Pharmacy, Chapel Hill, North Carolina

https://pharmacy.unc.edu/news/directory/drhoney/
For example medicine x ed purchase strattera 25mg amex, extend knee treatment 911 cheap strattera online master card, apply tubing behind medications you can take while nursing buy discount strattera 25mg line, and gradually allow tubing to medications jejunostomy tube buy cheap strattera on-line overcome resistance; end position of knee flexion. It may be that many chronic diseases and In the proliferative phase, arginine, glycine, proline, cancers are in part maintained or supported by this pro vitamins A and C, pantothenic acid, and zinc may inflammatory environment. Connective tissue repair may be aided One study indicates that women with high n6 fatty acid with glycosaminoglycans, manganese, and chon intake and a low n3 fatty acid intake were more prone to develop breast cancer. There is a belief that a ratio of n6 to n3 fatty acids should be close to 1:1 for humans to maintain an anti the Anti-Inflammatory Diet inflammatory internal environment. Ratios in the mod Linoleic acid from n-6 fatty acids is converted to ern diet can be as high as 10�30:1. The molecular mim sponses will occur icry theory is an extrapolation of the viral mimicry the ory that is believed to be the mechanism by which some diseases such as multiple sclerosis are activated. For example, bovine serum albumin prostaglandin E-2, decreasing or blocking inflammation. One suggested test for the Green tea polyphenols, resveratrol from red wine, vi leaky gut syndrome is the lactulose-manitol test. It is possible that caretonoids and ing intestinal lining includes (see Table 1�9): flavonoids also have similar actions. Dosage Special Instructions Possible Side Effects Glucosamine sulfate Stimulates the rebuilding 500 mg three times per day Take with meals No contraindications of damaged cartilage Take 6�8 weeks to determine May cause some gastrointesti effect nal upset Does not interfere with other anti-inflammatory drugs Some products processed with sodium chloride;use caution with patients who are hypertensive Boswellia Decreases inflammation 150 mg three times per day (for Take for 8 to 12 weeks None at recommended dosage example,if extract contains 37. Contraindicated in patients with bleeding tendencies (or peptic ulcer);systemic infection;or allergy to source product such as pineapple,pork,beef,or papaya. Herbs� Boswellia,ginger,tumeric,cayenne Boswellia� 400 mg,ginger� 300 mg,tumeric� 200 mg,cayenne� 50 mg taken every 2 waking hours during inflammatory phase. National Institute of Arthritis and Musculoskeletal Qualify each diagnosis with a description of whether and Skin Diseases acute, chronic, traumatic, non-traumatic, and in (877) 220-4267; If possible a more specific code should be in American Autoimmune Related Disease Association vestigated (search alphabetical index). Codes picture of the patient, and (2) when an underlying Palmer Chiropractic College West Clinics disease must be coded first. The reduction in the number of codes used intentional, inappropriate use to provide a patient is based on patient presentations commonly seen. This dis representation that is more conducive to reim tillation does not exclude the use of less common codes bursement by an insurance company when needed. The focus on more commonly seen presentations, associated codes and their operational def the lack of consistency is often based on a lack of under initions will assist in: standing regarding the use of codes. Not always clearly defined, but a clear set of criteria to define a given diagnosis. Also, not clearly defined, however, implied is the use of some codes only Realizing that, to some degree, the designation of a given when radiographic or special imaging confirmation is code or group of codes to a given patient presentation is available. Intertester reliability confirmation in addition to clinical information for their of the Cyriax evaluation in assessing patients with shoul use. Motion Palpation and Chiropractic 722�intervertebral disc disorders (includes disc Technique: Principles of Dynamic Chiropractic. Lumbar spine films in primary care: regions current use and effects of selective ordering criteria. Diagnostic imaging of the spine in chiropractic practice: recommendations for 756. Diagnostic imaging injury practice guidelines for musculoskeletal complaints in adults�an evidence-based approach: introduction. Observed changes in lateral abdominal muscle thickness after spinal manipula References tion: a case series using rehabilitative ultrasound imaging. Myofascial Dysfunction: the Trigger function and stress urinary incontinence: a case report ap Point Manual. Rehabilitative Ultrasound Imaging Sympo chemical milieu of human skeletal muscle. Rehabilitative ultra ated with pain and inflammation are elevated in sites near sound imaging: when is a picture necessary. Optimal methods for shoul ultrasound imaging: understanding the technology and its der tendon palpation: A cadaver study. London: Bal habilitative ultrasound imaging of pelvic floor muscle func liere Tindall; 1982. Manipulative Therapy in Rehabilitation of the Lo and mechanical compromise of peripheral nerves of the comotor System. Handbook of Preventive and Therapeutic Nutri Guidelines for Quality Assurance and Practice Parameters. Introduction Competence means among other things expertise, mastery, ability and proficiency. It includes essential knowledge, values and skills vital to the successful performance of effective practice of medical care. The emphasis in training is on �how to learn� rather than �how to be taught� and Teacher directed learning of the art and science of helping trainees to learn. Physical Medicine and Rehabilitation, also called Physiatry or Rehabilitation Medicine, is an independent clinical branch of medical science emphasizing the prevention, diagnosis, evaluation and treatment of disorders, particularly those of the neuro-musculo-skeletal, cardiovascular, and pulmonary systems, at any age, acquired or congenital, that may produce temporary or permanent activity limitation, disability, or participation restriction in society including loss of Quality of Life. This framework recognizes the underlying pathology, the level of organ functioning and the potential for restoring/optimizing personal function or preventing further limitation of activity. It also recognizes that the ability to participate depends not only on activities or personal functioning but also on a corresponding number of contextual factors affecting personal life and the individual�s environment. It has a vast scope since it provides integrated comprehensive care in the diagnosis, treatment and rehabilitation management of neurological, musculo-skeletal, cardio-pulmonary disabilities from acquired or congenital conditions presenting at any stage in life from pediatric to geriatric phases. This specialty focuses on the restoration of function of people to the highest possible level, through a multi disciplinary team approach, by a set of well planned interventions directed towards achievement of functional goals preset by the clinical investigation and evaluation by the team. This necessitates the utilization of diagnostic and therapeutic armamentarium including education and counseling, prescription of medicines, therapeutic exercises, equipments (mobility aids, orthotic-prosthetic appliances, assistive technology, physical agents and modalities, etc. It is also involved in disability prevention, evaluation and certification, besides development, monitoring and supervision of a rehabilitation plan and conducting research and development. The curriculum addresses the knowledge, skills, attitudes and competencies required to do this. The necessity of enhancing the number of such specialists is becoming more considering the epidemiological and demographic transitions and its antecedent high incidence and prevalence of chronic disorders and disabilities in the near future. Individual so afflicted has to become capable to live in the society with disability and also every society has to make provisions for the person with disability. The person trained should be able to identify, investigate, diagnose, confirm, evaluate, prognosticate, certify, treat, and rehabilitate, if and when a person is suffering from a temporary or permanent limitation in function, disability, or restriction in participation as well as plan, prescribe, monitor, supervise and lead the execution of rehabilitation plan through an integrated, multi-disciplinary team involving various medical, nursing, paramedical or allied health professionals such as therapists (occupational therapists, physiotherapists etc. He/she should be able to interpret reports and plan research, teach 5 medical and paramedical personnel, educate the person with disability, family, rehab team members and community, and be well versed with recent advances, administrative, financial, ethical and legal aspects related to the specialty. The clinical postgraduate training program is intended at developing in a student a blend of qualities of a clinical specialist, a teacher, a rehabilitation administrator and a researcher. They are organized in such a manner that a postgraduate should posses the following qualities and knowledge on qualification. It is expected that a new trainee will have acquired and will continue to develop competencies that ensure the highest standard of patient care. These competencies are described as learning objectives with specific knowledge and skills. These attitudes are: Persons with Disability Focus A Physiatrist: 6 � has a positive and constructive attitude to the development of strategies to enable the person with disability and activity limitation or participation restriction to realise their full potential � recognises the perspective and beliefs of the patient, and endeavours to incorporate the patient�s needs and expectations into the plan of care � is aware of and sensitive to issues of ethnicity, culture, gender and sexuality � recognises the importance of the family and other carers in supporting the patient, as well as the potential difficulties the family may experience in the care of a family member with a disability. Professional Role A Physiatrist: � behaves with empathy, courtesy, responsibility and accountability towards patients and their families, and towards other health professionals � understands the extent of their competence and how their role extends the traditional medical role � recognises and respects the contributions and roles of other medical practitioners in the process of care � is prepared and willing to promote rehabilitation medicine actively to the medical profession. Continuing Professional Development A Physiatrist: � views competence as a continuing process of education and learning by which he/she ensures that clinical practice is of the highest standard � is willing to review personal competence openly and regularly, and to improve clinical skills as necessary. Interdisciplinary Management 7 While a Physiatrist accepts full and ultimate responsibility for the rehabilitation care of the patient, he/she: � recognises the appropriateness of interdisciplinary team management, especially in the care of persons with permanent and complex disability � understands the specific skills of each team member, and develops a close professional relationship with these allied disciplines � appreciates the synergistic effect of cohesive team management, and strives to support the team in achieving holistic and expert care. Advocacy A Physiatrist is: � prepared at all times and to the best of his/her ability to represent and support persons with disability in the achievement and defense of their rights to receive optimal medical and rehabilitation care, and to pursue their chosen lifestyle with independence and dignity � aware of the full extent of potential disadvantage arising from disability, and is willing to assist persons with disability in achieving their full rights in society, especially with regard to medical care, accommodation, community support, community access, safety, transport, and appropriate political and legal representation. He/ she should be able to practice and handle independently most day to day problems as encountered in Physical Medicine and Rehabilitation. He/ she should also be able to recognize the need to seek further help, when required. Given adequate opportunity to work on the basis of graded responsibilities in out-patients, in-patients and operation theatre on a rotational basis in the Department from the day of entry to the completion of the training program the students should be able to: a) Acquire scientific and rational approach to the diagnosis of cases presenting b) Acquire understanding of and develop inquisitiveness to investigate to establish the cause and effect of disease, disability and activity limitation as well as participation restrictions c) Prescribe all routine and special investigations pertaining to the specialty and interpret the results of these and other investigations in the light of clinical presentation d) Manage and treat all types of cases in Physical Medicine and Rehabilitation that occur commonly e) Demonstrate knowledge of the pharmacological aspects of drugs/ medicines used in various forms and through various routes, in Physical Medicine and Rehabilitation f) Competently handle and execute safely all the routine/ essential rehabilitative surgical procedures g) Demonstrate understanding of the fabrication and competence in prescription and check out of orthoses and prostheses as well as various assistive devices and mobility aids 9 h) Understand the principles, prescription and supervision of physiotherapy, occupational therapy, speech therapy and medico-socio-vocational-psychological counseling (iii)Environment and Health: He/ she should understand the effects of environment on health and be familiar with the epidemiology of common diseases presenting in the field of Physical Medicine and Rehabilitation. He/ she should be able to integrate the preventive and promotive methods along with the curative and rehabilitative measures in the treatment of diseases.
Objectives 2 Through efficient treatment 5 shaving lotion purchase 25mg strattera visa, focused symptoms for pregnancy discount strattera 25 mg with visa, data gathering: � Determine whether an increase in water relative to medications causing hair loss purchase strattera 40mg otc sodium exists thereby expanding volume of cells or the change in sodium concentration is artifactual or caused by hyperglycemia medicine x stanford discount strattera 40mg with visa. When serum sodium concentration is measured by flame photometry or other methods requiring major dilution of plasma, hyperlipidemia or hyperproteinemia may cause pseudo-hyponatremia (iso-osmotic). Explain how serum sodium concentration represents the major determinant of extracellular osmolarity and how its level of 135 145 mmol/L is controlled. Contrast the mechanism of water retention when water intake is great enough to overwhelm the excretory capacity of the kidney to water retention caused by impaired renal water excretion. Sore throat may be due to a variety of bacterial and viral pathogens (as well as other causes in more unusual circumstances). Infection is transmitted from person to person and arises from direct contact with infected saliva or nasal secretions. Rhinorrhea alone is not infective and may be seasonal (hay fever or allergic rhinitis) or chronic (vaso-motor rhinitis). Such patients usually have a viral upper respiratory infection and do not require diagnostic tests or treatment. Objectives 2 Through efficient, focused, data gathering: � Determine whether further testing for group A streptococci is indicated (or other investigation). Sore throat is one of the commonest conditions found by physicians in office practice and emergency departments. Although the major treatable pathogen is group A streptococcus, this organism is the cause of the sore throat in<10% of adults who present with this complaint. Unfortunately, the majority of patients continue to receive presumptive antibiotic therapy for this complaint. Almost of adults presenting to family physicians in office practice are prescribed antibiotics. In many of these instances, the antibiotics are the more expensive broad-spectrum agents despite the fact that such practice is not consistent with recommended practice guidelines. In other words, over-treatment of this condition represents one of the major causes of antibiotic abuse. Outline the rationale for testing for any of these organisms and indicate the tests currently available. If the specificity and sensitivity of rapid tests for these agents were given, indicate how it would/would not influence your decision regarding therapy. List tests available to determine whether the sequel to one of these infections has developed. This means that in addition to the roles specialists may have, the family physician must play an important role. Congenital and other (septal deformity, choanal atresia, vestibular stenosis, foreign body) 2. Other (neoplasia benign/malignant, chemicals, drugs) Key Objectives 2 Before initiating an extensive evaluation, confirm the fact that the subjective complaint of smell or taste loss truly represents a derangement of smell (total loss of taste is rarely seen because of the anatomy of the taste system). One of the more common causes of abnormal growth is mis-measurement or aberrant plotting. Tall stature (children develop pituitary gigantism; adults are not taller, but have acromegaly) a. Excess other Hormones (precocious puberty [tall early, later short], thyroid) iii. Accelerated early growth, more accelerated epiphyseal closure (precocious puberty) Key Objectives 2 Determine whether growth progressively deviates from previously defined percentiles. Objectives 2 Through efficient, focused, data gathering: � Elicit history of uterine growth rate, intrauterine infections, maternal exposure to toxins, smoking, alcohol, or systemic illness. Amblyopia without strabismus Key Objectives 2 Determine the type of strabismus and the necessary timing of intervention. Objectives 2 Through efficient, focused, data gathering: � Differentiate pseudo strabismus (lid configuration or negative angle kappa or markedly positive angle kappa) from true strabismus; obtain relevant family history. Moreover, 10 15% of outpatient visits as well as 25 40% of hospital admissions are related to substance abuse and its sequelae. Other (ketamine) Key Objectives 2 Determine whether the patient is in need of emergency care because of withdrawal symptoms or other complications. Objectives 2 Through efficient, focused, data gathering: � Determine past and recent quantity and frequency of abuse, severity of abuse and dependence, readiness to change or denial, complications of use, family history, past treatment history, support network, and withdrawal symptoms; identify social problems such as assault and impaired driving. It is imperative that the precursors, probable cause and parental concerns are extensively evaluated to prevent recurrence. Suicidal behaviour is one of several psychiatric emergencies which physicians must know how to assess and manage. Objectives 2 Through efficient, focused, data gathering: � Elicit history of risk factors, suicidal thoughts, content and duration, frequency, plan, and rehearsal. There are several ethical principles that some will argue to justify physician-assisted suicide or euthanasia, while others will provide counter arguments. It can be argued that it is for the patient to decide whether they wish to end their own life. The counter argument is that autonomy does not permit the voluntary ending of the conditions necessary for autonomy. Since death would end the possibility of autonomy, it cannot justify euthanasia or physician assisted suicide. However, research indicates that most patients requesting euthanasia are not the ones suffering unbearable pain. Moreover, with the improvement in end of life care, it is extremely rare that pain or other forms of suffering cannot be controlled. As a consequence, it is difficult to justify a general approach such as euthanasia to furthering well-being when in fact this well-being would apply to extremely few and many others, because of the marked improvement in end of life care, are no longer suffering. Another argument in favor of euthanasia is that there is no difference between stopping life-sustaining treatment and euthanasia. Others will argue that what is different is the intention: removal of invasive treatment rather than ending of life. Finally, an argument against physician assisted suicide and euthanasia is the so-called "slippery slope" argument. Evidence for this is not very convincing, but the Netherlands experience should be considered. In summary, if a physician is requested to provide assistance toward ending life, the physician should reassure the patient that under no circumstance is the patient going to be abandoned. The physician should tell the patient that continuous care will be provided indefinitely. The physician should also consider early psychiatric referral since patients interested in euthanasia are more likely to be depressed than suffering unbearable pain. Physicians are required to distinguish syncope from seizures, and benign syncope from syncope caused by serious underlying illness. Psychiatric (panic disorder, hysteria, hyperventilation) Key Objectives 2 Differentiate syncope from disturbances of cerebral function caused by a seizure (patients with seizure rarely have an abrupt and complete recovery). Objectives 2 Through efficient, focused, data gathering: � Differentiate between cardiac and non-cardiac causes. Since consciousness in part depends on perfusion of the brain, discuss autoregulation of cerebral blood flow. Outline the relationship between blood pressure, cardiac output, and systemic vascular resistance; the relationship between cardiac output, stroke volume and heart rate; the relationship between stroke volume, contractility, preload, and afterload; the relationship between preload, intravascular volume and vascular capacitance. It is a medical emergency and may be associated with severe complications and death. Impaired thermoregulation, neurologic (hypothalamic/cerebral stroke, status epilepticus) b. Malignant hyperthermia/Genetic, increased myocyte metabolism after anesthetic iii. Neuroleptic malignant syndrome, increased myocyte metabolism + altered thermoregulation (anti-psychotics:phenothiazines,haloperidol) 2. Drugs (anticholinergic, sympathomimetic, diuretic, salicylate toxicity, serotonin syndrome) 3. Objectives 2 Through efficient, focused, data gathering: � Elicit a history of chronic medical conditions that either impair thermoregulation or prevent removal from a hot environment, heavy exercise in high ambient temperatures, anesthetics, or anti-psychotics. Contrast increased heat load to diminished heat dissipation; contrast heat load absorbed from environment to metabolic heat.
The dihydropyridine receptors communicate with the ryanodine receptors of the sarcoplasmic reticulum medicine 101 order cheap strattera line, a mechanism poorly understood symptoms 4dp5dt fet purchase strattera without a prescription. Calcium is released from the sarcoplasmic reticulum through the ryanodine receptors medications you can take while pregnant for cold generic 40mg strattera amex. Calcium binds to medicine mart purchase discount strattera line the regulatory protein, troponin C, and the interaction between actin and myosin can occur. The myosin cross-bridges move into a strong binding state, and force production occurs. Muscle spindles provide sensory information concerning changes in the length and tension of muscle fibers. Their main function is to respond to the stretch of a muscle and, through reflex action, to produce a stronger contraction to reduce the stretch. The spindle is fusiform in shape and is attached in parallel to the regular or extrafusal fibers of the muscle. There are two sensory afferents and one motor efferent innervating the intrafusal fibers. The gamma efferent innervates the contractile portion�the striated ends of the spindle. These fibers, activated by higher cortex levels, provide the mechanism for maintaining the spindle at peak operation at all muscle lengths. When skeletal muscles contract voluntarily against a load, motor units are recruited from smallest to largest. Connected in series to 25 extrafusal fibers, these sensory receptors also are located in the ligaments of joints and are primarily responsible for detecting differences in muscle tension. The Golgi tendon organ functions as a protective sensory mechanism to detect and inhibit subsequently undue strain within the muscle-tendon structure. Describe the adaptations in muscle structure that occur with progressive resistance exercises. The major adaptation is an increase in the cross-sectional area of muscle, which is termed hypertrophy. Progressive resistive exercise involves 10 repetitions a day at 60% to 90% of maximal capacity; this results in an increase in strength by 0. There are increases in the amounts of transverse tubular and sarcoplasmic reticulum membranes as well. Furthermore, neural adaptations result in an increased ability to recruit high-threshold motor units. The functional significance of this morphologic change is primarily a greater capacity for strength and power development. Endurance exercise has minimal impact on the cross-sectional area of muscle and muscle fibers. The smaller cross-sectional area allows better diffusion of metabolites and nutrients between the contractile filaments and the cytoplasm and between the cytoplasm and the interstitial fluid. The number of capillaries increases around each fiber, and there is an increase in mitochondria, especially in the type I fibers. The more extensive capillary bed improves the delivery of oxygen and circulating energy sources to the fibers, whereas the products of muscle activity are removed more efficiently. The functional significance of these changes is observed during sustained exercise, in which there is a delay in the onset of fatigue. Sarcopenia is the term used to describe age-related loss of skeletal muscle mass and strength. This form of skeletal muscle atrophy is systemic and associated with metabolic and/or inflammatory factors. Apoptosis, or programmed cell death, is a regulated physiologic process critical to cellular homeostasis, which can become dysregulated, leading to disease states including muscle disease or dysfunction. Necrosis is a pathologic process caused by the progressive degradative action of enzymes that is generally associated with severe cellular trauma in muscles, leading to cell death. Skeletal muscle structure, function, & plasticity: the physiological basis of rehabilitation (3rd ed. Molecular diversity of myofibrillar proteins: Gene regulation and functional significance. Sarcopenia is the term describing the loss of muscle mass and strength with aging. The physical activity level does not affect the changes of skeletal muscles with aging. Fast-twitch muscles show more significant age-related changes than slow-twitch muscles 2. Although two movements may appear similar (kinematics), the underlying forces causing those movements (kinetics) may be very different. This fact should be appreciated when using readily available motion analysis tools (such as recording movements on smartphones or tablets). Impulse is the area under the force-time curve and accounts not only for the magnitude of the force but also for the duration over which the force is applied. Impulse determines the change in a body�s momentum, which is the product of mass and velocity. Applying a smaller force over a longer period of time will have the same impulse (and effect on a body�s momentum) as applying a larger force over a shorter period of time. Increasing the time of the impact, which can be accomplished by cushioned shoes and/or bending the knees when making contact with the ground, can attenuate the magnitude of an impact force and may decrease the risk of injury. Elastic materials, such as bands and tubes, are often used as a form of resistance and follow Hooke�slaw (the force is proportional to the stiffness and elongation). The stiffness is determined by the manufacturer (whichusesdifferentcolorsfordifferentlevelsofstiffness)andwilldecreasewithtimeasthematerialfatigues. It is also important to keep in mind that the elongation is related to the resting length of the band or tube and not just the elongation during the exercise. In the first, an exercise starts with the band at its resting length and is elongated by a certain amount, �x. What is the relation between the linear motion at the joint surface and the angular motion of a bone around the joint axis A theoretical construct, developed to describe this relation and advocated by Kaltenborn, is known as the convex-concave rule. In brief, if the convex surface of one bone is moving on the fixed concave surface of another bone, rotation and translation will occur in opposite directions. Additionally, if the concave surface of one bone is moving on the fixed convex surface of another bone, rotation and translation occur in the same direction. It is proposed that in order to restore rotational motion at a joint, a linear mobilization is performed in relation to the treatment plane, which is parallel to the concave joint surface. Mobilization can be performed on either segment in accordance with the convex-concave rule. For example,it has beendemonstratedthatthe glenohumeraljoint contradicts the convex-concave rule during external rotation when the humerus is abducted to 90 degrees, and there is no clear consensus that the femur translates anteriorly when the knee is flexing in a weight bearing position. However, these findings may not violate the convex-concave rule if the amount of translation in the direction of rolling is less than what the curvature of the convex segment would predict. The amount of rolling in one direction may be greater than the sliding in the opposite direction. Therefore the application of the convex-concave rule to treatment may need to be further informed by the direct method of assessing a restriction of joint gliding. To reflect that change, the axis (or center) of rotation is called the instantaneous axis (or center) of rotation. Cartilage degeneration often accompanies the presence of a nonfixed axis of rotation. An absolute angle is the angle that the distal point of a segment (eg, foot, shank, thigh) makes with respect to some reference line (such as the horizontal for sagittal plane movements). A relative angle is the joint angle made by two segments (eg, the knee angle is the angle between the shank and thigh). Relative angles can be stated as either internal (included) or external (anatomic) angles.
Proteins Only a limited number of protein functions could be predicted by similarity searches symptoms of ebola discount strattera 18mg on-line. Eight inser tions/deletions are present and 88% of the encoded gene products are related treatment concussion buy 18 mg strattera with visa. These phage also share a strikingly conserved order of structural genes suggesting that these features are of very ancient origin medicine 74 cheap strattera 25 mg without prescription. Genus �n4-like viruses� Type species Escherichia phage N4 Virion properties morPholoGy Virions have icosahedral heads about 70 nm in diameter and short tails 10 nm in length medications via g-tube buy strattera 18 mg on line, with several short fbers originating from the junction between the head and tail (Figure 4). Early and middle genes occupy a contiguous block in the left half of the genome and are transcribed rightwards. Physicochemical and Physical ProPerties Virion buoyant density in CsC1 is about 1. Other members of the genus have genome sequences of 38�42 kbp with similar organization and similar transcriptional programs. Proteins P22 virions contain nine structural proteins: 415 copies of the major capsid protein (gp5; 46. Genome organization and replication the P22 genetic map is circularly permuted, has terminal repeats of about 1600 bp (3. Other genus members have similar but different relationships with other �lambda-like viruses�. Transcription starts with regulatory genes and pro ceeds in three partly overlapping waves that are very similar to those of the lambda-like viruses. Replication starts at a single site and involves replication by a (theta) structure mechanism that switches at late times to a rolling-circle mechanism (, sigma replication). Biological properties Phages are temperate and can carry out generalized transduction with lysogenic conversion ability. Members of the genus infect Enterobacteria (Escherichia, Salmonella and other Gammaproteobacteria) and have, under suitable conditions, very high (up to 500) burst sizes. Virion properties morPholoGy this virus displays C3 type morphology with an elongated head (ca. Figure 6: Electron micrograph of phiEco32 stained with phosphotungstate in the presence of bacitracin. List of other related viruses which may be members of the genus �Phieco32-like viruses� but have not been approved as species Recently Salmonella phage 7-11 was sequenced and suggested as a member of this genus. Based on comparative proteomics data, this grouping was established as a subfamily. More importantly, these phages share a common general genome organization, with genes encoded solely on the Watson strand. Within this subfamily, distinctive features warrant a separation into different genera. The same argument can be given for marine bacteriophage VpV262 infecting Vibrio parahaemolyticus. Virion properties morPholoGy Phage morphology is conserved compared to �T7-like viruses� and consists of a short tail and an icosahedral capsid of about 60 nm in diameter. The structural (virion-associated) peptidoglycan hydrolase domain, located at the C-terminus of the predicted internal protein gp36, has a high refolding capacity and is thermoresistant. Biological properties Phages are highly virulent with a short infection cycle, and infection typically leads to the formation of large (ca. Although there are substantial similarities to the T7-like viruses, there are key proteomic differences shown by CoreGenes analysis. The tail is short and stubby (like T7) and has been described as possessing an �irregular bushy structure�. Physicochemical and Physical ProPerties Infectivity is ether and chloroform-resistant. Proteins Structural proteins have been predicted based on the relationship to other phage in the subfamily Autographivirinae. Species demarcation criteria in the genus Species are separated by host range and supported by proteomic analyses. Virion properties morPholoGy T7 phage heads are icosahedra, measure about 60 nm in diameter, and consist of 72 capsomers (60 hexamers and 12 pentamers; T 7). Physicochemical and Physical ProPerties T7 virion Mr is about 48 106, buoyant density in CsCl is 1. Molecular Biology, Science Books International, Boston, and Van Nostrand Reinhold, New York, p. Genome organization and replication the T7 genetic map is linear, non-permuted and terminally redundant, and comprises about 55 genes, several of which overlap. Infection results in shut-off of host syntheses and a breakdown of the host genome. Replication is bidirectional and produces concatemers by end-to-end join ing of intermediate forms. Biological properties Phages are virulent and are specifc for enterics and related Gram-negative bacteria. Picovirinae refers to the small (Pico-) virion and genome sizes of the viruses within this subfamily, which represent the smallest tailed phages known. The evolutionary link to the �Phi29-like viruses� is clearly present throughout the subfamily, both morphologically and molecularly, since all these phages also contain a type B polymerase, apart from other similar gene products and overall genome size. From this perspective, phages Actinomyces phage Av-1, Streptococcus phage Cp-1 are included within this subfamily but not assigned to a particular genus. This needs confrmation since we may be observing a case of genome size reduction (as shown by Mycoplasma hosts themselves). Virion properties morPholoGy Isometric phages, with short, non-contractile tails and a pre-neck appendage. Metabolism-related genes are encoded on the Watson strand of the genome, whereas genes encod ing structural proteins are located on the Crick strand, separated by a bidirectional terminator. Genus �Phi29-like viruses� Type species Bacillus phage phi29 Virion properties morPholoGy Heads are prolate icosahedra (T 3 with 30 hexamers and 11 pentamers) and measure about 54 42 nm. Some members, including Bacillus phage 29, have about 55 fbers on the head (Figure 9). Tails measure 46 8 nm; have a distal thickening, and a collar with 12 appendages. Physicochemical and Physical ProPerties 29 virion Mr is 29 107, buoyant density in CsC1 is 1. Proteins Virions have nine structural proteins (13-86 kDa), including 235 copies of the major capsid protein (49. Genomes are non-permuted and have inverted terminal repeats from 6 to 8bp (Phi29) to 230�240 bp (Cp-1). Early genes are transcribed from right to left on the standard map (except in Cp-1 where some are from left to right); late genes are transcribed from left to right. Biological properties Phages are virulent and infect Gram-positive bacteria with low G C contents. In addition, phages 29 and Cp-1 have opposite directions for transcription of early genes at the left end of the chromosome. See �Similarity with other taxa� in the Caudovirales description for further details. Molecular and physiological analysis of three Pseudomonas aeruginosa phages belonging to the �N4-like viruses�. Genomic sequence and evolution of marine cyanophage P60: a new insight on lytic and lysogenic phages. Backbone structure of the infectious 15 virus capsid revealed by electron cryomicroscopy. The genome of 15, a serotype-converting, Group E1 Salmonella enterica-specifc bacteriophage. The genome sequence of enterobacterial phage 7-11, which pos sesses an unusually elongated head. The structures of bacteriophages K1E and K1-5 explain processive degradation of polysaccharide capsules and evolution of new host specifcities. P22 coat protein structures reveal a novel mechanism for capsid maturation: stability without auxiliary proteins or chemical crosslinks.
Discount strattera 10 mg free shipping. Causes Symptoms and Treatment of Pneumonia.