

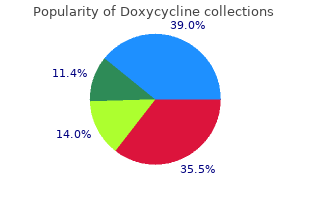
Doxycycline
"Buy doxycycline 200mg cheap, antibiotic pseudomonas."
By: Randolph E. Regal, BS, PharmD
- Clinical Associate Professor, Department of Clinical Pharmacy, College of Pharmacy, University of Michigan
- Clinical Pharmacist, University of Michigan Health System, Ann Arbor, Michigan

https://pharmacy.umich.edu/people/reregal
Depressed individuals commonly complain of early morning awakening or may appear to antibiotic 500g cheap doxycycline 100 mg amex sleep most of the night but not feel rested in the morning peg 400 antimicrobial cheap 100mg doxycycline amex. There are no ideal hypnotic medications hpv virus generic doxycycline 200 mg with amex, but agents such as sedating antidepressants (such as trazodone) or neuroleptics (such as quetiapine) may be used judiciously antibiotic resistance video doxycycline 200 mg on-line. Benzodiazepine and other prescription sedative-hypnotics are potentially delirogenic and habit forming and should be used cautiously, if at all. This may be acceptable to the person and family if it is understood as a feature of the disease. In situations where harm could result from apathy, for example if the person is not getting out of bed for meals, judicious use of amphetamines may be appropriate. The person experiences the failure of his hopes for the future and the loss of his sense of self worth and begins to experience despair. Demoralization should be considered when the person lacks the full depressive syndrome, and when the feelings of hopelessness have arisen in clear proximity to signifcant losses. Treatment for demoralization requires a combination of psychotherapy and social work to help the individual, and his or her family, solve real world problems, reduce stressors, build a support system, and emphasize the positive factors in life. His disability pension is fairly generous and his wife picks up extra hours at her job to make ends meet. Now that he is home, however, he is not helping with the household chores, is irritable with his wife and children and is beginning to drink excessively in the evenings. He tells his wife that he feels worthless and “half a man” and she is worried because he still owns a revolver. He seems surprised at the question and replies that he would never do such a thing to hurt his family. He discusses his feelings of guilt and worthlessness over not being able to provide for his family. The doctor reminds him that his condition is very mild and that he has many good years ahead of him. He agrees to abstain from alcohol for the time being and, with encouragement, obtains a part time job providing security at a large retail store. With the money he is making, his wife is able to reduce her hours and now that he is feeling less resentful, he begins to pitch in at home, going grocery shopping or doing the laundry. Six months later, at a follow- up visit, he is in excellent spirits and has made a successful transition to his new situation. This may be due to the onset of symptoms in the child before the parent’s onset, the early death of a parent (before the parent’s symptoms were evident), misdiagnosis or lack of diagnosis in a parent who was affected, non-paternity (a biological father who is not the same as the apparent father), or adoption. However purchase ceftin 250mg on line, some people do develop non-specific symptoms at times when the virus is reproducing and causing liver problems ceftin 500 mg for sale. People with lifelong hepatitis B infection can develop cirrhosis of the liver generic ceftin 500 mg fast delivery, liver cancer order ceftin paypal, and/or liver failure, which can lead to death. An exposure is defined as contact with blood or other body fluids of an infected person. Contact includes touching the blood or body fluids when you have open cuts or wounds (that are less than 24 hours old or wounds that have reopened), splashing blood or bloody body fluids into the eyes or mouth, being stuck with a needle or other sharp object that has blood on it, or having sex or sharing needles with someone with hepatitis B virus. Everyone who has an exposure to a person infected with hepatitis B virus should have blood tests done as soon as possible to determine whether treatment is needed. In some cases, people who have already been vaccinated may be tested and/or revaccinated. If a mother develops hepatitis B during her pregnancy, there is a chance that the baby may also become infected. If the mother develops acute hepatitis in the third trimester of pregnancy or the immediate postpartum period, the risk of infection for the newborn baby may be 60% to 70%. It is very important that the baby receive treatment right after birth to get as much protection as possible. They may have the virus for the rest of their lives and be a source to spread the disease. All pregnant women should be tested for hepatitis B virus early in their pregnancy. Check with your healthcare provider for the schedule for dose 2 and dose 3 of the vaccine. Once the baby has turned 1 year of age, the baby should have a blood test to make sure infection did not occur and that the vaccine is protecting the baby. The blood test for hepatitis B may show that you: Are immune (had hepatitis B disease or vaccine in the past) and have no sign of recent infection. You should receive the hepatitis B vaccine series if you are at risk of blood exposures at your job or through risk behaviors in your personal life. Is there a way I can keep from being infected with hepatitis B during my pregnancy? In adults, the virus is most often spread through sexual contact or by sharing needles. Although it is rare, there are some children who become infected with the virus from their infected mothers during pregnancy, at the time of birth, or through breastfeeding. An exposure is defined as direct contact with the blood or body fluids of an infected person. The test should be repeated 3 months and 6 months after exposure to completely rule out infection. About 25% of babies of infected mothers who do not receive antiretroviral treatment may become infected, whereas, about less than 2% become infected when the mother receives antiretroviral treatment. The infant can become infected anytime during pregnancy, but infection usually happens just before or during delivery. An infant may be tested as early as 48 hours and may be tested periodically for up to 2 years. For this test to be accurate, it should be conducted a minimum of three weeks to three months after a known exposure. Symptoms include generalized skin rash, tiredness, headache, fever, and swollen glands in the area behind the ears and the neck (lymphadenopathy). It is estimated that 25% to 50% of persons infected with rubella may not have any symptoms. However, there may be severe illness in adults who have not had the disease in the past or have not had the vaccine. Joint stiffness and/or joint pain may occur in up to 70% of adult women infected with rubella. Some of the other problems that may occur include a bleeding problem called thrombocytopenia and infection of the brain (encephalitis). After the 20 week of pregnancy if a woman develops rubella, most likely there will not be any problems for either the mother or the unborn baby. If you know that you are immune to rubella (had a blood test to show that you have antibodies to rubella), you do not need to be concerned about the exposure. If you are not immune to rubella and have been exposed to someone with rubella or have developed a rash illness that might be rubella, you should call your healthcare provider. The blood test for rubella may show that you: Are immune (had rubella disease or vaccine in the past) and have no sign of recent infection. You should discuss what the risks are based on your stage of pregnancy with your healthcare provider. If you are not pregnant and not immune, all adults working with children should know their vaccine history or immune status. When you are given the vaccine you should avoid becoming pregnant for at least one month after immunization. Varicella-zoster is a herpes virus that causes chickenpox, a common childhood illness. After a person has had chickenpox, the varicella-zoster virus can remain inactive in the body for many years. The sores commonly occur in batches with different stages (bumps, blisters, and sores) present at the same time. A person with chickenpox is contagious 1-2 days before the rash appears and until all blisters have formed scabs. Children with weakened immune systems may have blisters occurring for a prolonged time period. Shingles occurs when the virus, which has been inactive for some time, becomes active again. Severe pain and numbness along nerve pathways, commonly on the trunk or on the face, are present. The blisters are usually on one side of the body and closer together than in chickenpox.
Syndromes
- Do not bathe or wash your hair often
- Did the paleness develop suddenly?
- Take medicines to treat reflux disease (heartburn), if you have it.
- Allergic reaction to the contrast dye
- When you sleep, do not lie on the side that has bursitis. Place a pillow between your knees when you lie on your side to help decrease your pain.
- Blood tests such as a complete blood count (CBC)
- Abnormal urine color (cloudy urine)
The accurate bacteria helicobacter pylori sintomas cheap doxycycline 200mg with amex, sensitive and reproducible method for the quantitation of pefloxacin in plasma antibiotics for uti new zealand buy cheap doxycycline 100 mg on-line. Bioequivalence Food and Drug Administration antibiotic resistance vets discount doxycycline online american express, Division of Bioequivalence Bioequivalence Food Drug Administration Fda Guidelines Bioequivalence Food and Drug Administration virus 57 order generic doxycycline on-line. Bioequivalence Food and Drug Administration, Division of Bioequivalence Bioequivalence Food Drug Administration Bioequivalence Food and Drug Administration. Single doses of norfloxacin (200, 400, 800, 1,200, and 1,600 mg) or placebo were administered orally at weekly intervals to 14 healthy male volunteers in a double-blind study. The concentrations of this drug in serum peaked 1 to 2 h after each dose; the mean peak values for increasing doses were 0. Mean area under the serum concentration-time curves for the first 12 h after each dose were 3. The elimination half-life of norfloxacin was about 7 h and was similar for all doses. The concentrations of the drug in urine also peaked 1 to 2 h after dosage; mean peak values for increasing doses were 200, 478, 697, 992, and 1,045 micrograms/ml. Crystals of the drug were occasionally observed during microscopic examination of freshly voided urine collected after the 1,200- and 1,600-mg doses. The early quinolones had a limited spectrum of activity, low potency, high frequency of spontaneous bacterial resistance, low serum drug concentrations and short half-lives, which virtually restricted their use to urinary tract infection. The new fluorinated quinolones differ from their predecessors in their broad antibacterial spectrum, including both Gram-negative and Gram-positive aerobic, and facultative anaerobic bacteria as well as many Mycobacterium spp. They also exhibit high potency, a low incidence of resistance, high oral bioavailability, extensive tissue penetration, low protein binding and long elimination half-lives. They are generally well tolerated apart from some gastrointestinal disturbance and rashes, including photosensitive eruptions and a propensity to cause central nervous system excitation. Clinically important interactions include those with antacids, theophylline, fenbufen and warfarin. Potential toxic effects include cartilage damage, ocular toxicity, teratogenicity and impairment of spermatogenesis. The role of fluoroquinolones continues to widen, encompassing infections of the urinary tract, respiratory tract, skin and soft tissues, bone and joints, infections in immunocompromised patients, sexually transmitted diseases, infectious diarrhoea, gynaecological infections and surgical prophylaxis. The convenience of oral therapy is an added advantage of the new fluoroquinolones. Suppose that a test formulation and a standard formulation are to be compared in an experiment with a two period crossover design. Suppose that it is desired to obtain a confidence interval for the ratio of the test formulation mean to the standard formulation mean for some variable. A method has previously been given for obtaining an exact confidence interval under a more restrictive model. Seven healthy subjects received, after an overnight fast, a single 200-mg oral dose of norfloxacin with water, whole milk, and unflavored yoghurt. Coadministration of milk or yoghurt reduced the extent of norfloxacin absorption and the mean peak concentration in plasma by approximately 50%. In bioequivalence assessment, the consumer risk of erroneously accepting bioequivalence is of primary concern. In order to control the consumer risk, the decision problem is formulated with bioinequivalence as hypothesis and bioequivalence as alternative. In the parametric approach, a split into two one-sided test problems and application of two-sample t-tests have been suggested. Rejection of both hypotheses at nominal alpha-level is equivalent to the inclusion of the classical (shortest) (1-2 alpha) 100%-confidence interval in the bioequivalence range. This paper demonstrates that the rejection of the two one-sided hypotheses at nominal alpha-level by means of nonparametric Mann-Whitney-Wilcoxon tests is equivalent to the inclusion of the corresponding distribution-free (1-2 alpha) 100%-confidence interval in the bioequivalence range. This distribution-free (nonparametric) approach needs weaker model assumptions and hence presents an alternative to the parametric approach. Statistical methods to assess bioequivalence of a test and a reference formulation are reviewed with emphasis on the distribution of bioequivalence characteristics and the consumer risk of erroneously accepting bioequivalence. Among the procedures not exceeding a nominal consumer risk of 5%, the one with an acceptably small producer risk of erroneously rejecting bioequivalence is selected. With the exception of tmax, the following strategy is recommended: a decision in favour of bioequivalence is made if the shortest 90%-confidence interval for the ratio of the expected medians is in the bioequivalence range for the chosen characteristics of rate and extent of absorption. If the assumption of a logarithmic normal distribution is not valid, the analogous nonparametric (distribution-free) 90%-confidence interval, which is also based on the two-sample approach for the sequences reference/test and test/reference, is the procedure of choice. Norfloxacin is an oral fluoroquinolone antimicrobial agent recently released for the treatment of uncomplicated and complicated urinary tract infections. Norfloxacin is more potent and broader in spectrum than the earlier developed analogue, nalidixic acid, and is active in vitro against virtually all bacterial pathogens causing urinary tract and gastrointestinal infections, aerobic gram-negative bacilli causing sepsis in neutropenic patients, and Neisseria gonorrhoeae. The drug is administered orally twice daily and achieves high concentrations in urine, stool, renal tissue, and bile. Norfloxacin was at least as effective as currently used agents in treating urinary tract infections, and, in limited studies, bacterial gastroenteritis, gonorrhea, bacterial prostatitis, and prevention of gram-negative bacillary infection in neutropenic patients. Adverse drug effects were mild and included disturbances of the gastrointestinal tract and the central nervous system. Norfloxacin shows promise as an antibacterial agent for genitourinary and gastrointestinal infections. The statistical test of hypothesis of no difference between the average bioavailabilities of two drug formulations, usually supplemented by an assessment of what the power of the statistical test would have been if the true averages had been inequivalent, continues to be used in the statistical analysis of bioavailability/bioequivalence studies. In the present article, this Power Approach (which in practice usually consists of testing the hypothesis of no difference at level 0. The only cases where the power approach has superior properties when the true averages are equivalent correspond to cases where the chance of concluding equivalence with the power approach when the true averages are not equivalent exceeds 0. With appropriate choice of the nominal level of significance of the one-sided tests, the two one-sided tests procedure always has uniformly superior properties to the power approach. The two one-sided tests procedure is compared to the procedure proposed by Hauck and Anderson. Saliva, throat and faecal specimens were collected days 0, 3, 5, 7, 14 and 21 to study the effect of norfloxacin on the normal microflora. No accumulation in faeces was found during the administration period, and mean concentrations were 940 mg/kg. The changes in the oropharyngeal flora were minor and only branhamella were affected. In the colonic flora, the number of enterobacteria was strongly depressed while the anaerobic microflora was only slightly affected. Two weeks after the administration period, both the oropharyngeal and colonic microflora had returned to normal. It is also shown that the use of norfloxacin can reduce the total number of bacteria at the site of an infection as well as having significant effects upon the metabolism of treated cells in the interim period between the loss of viability and cell-lysis. These effects may provide a clue to a previously unsuspected mechanism of providing symptomatic relief which functions in parallel with the elimination of viable pathogenic bacteria. In contrast 134 enterobacteria, 5 acinetobacter and all the pseudomonas and Gram-positive cocci were nalidixic acid-resistant. Sixty-two per cent of enterobacteria were inhibited by Norfloxacin is a quinolinecarboxylic acid compound. We examined the in vitro activity of this compound against gram-positive and -negative species, including anaerobic species. Yersinia, Arizona, and Aeromonas all were inhibited at concentrations below 1 microgram/ml, as was Campylobacter. The activity of norfloxacine was not affected by the type of medium, pH, or inoculum size. Norfloxacin inhibited bacteria in every species which was resistant to ampicillin, carbenicillin, cephalexin, gentamicin, and trimethoprim at concentrations lower than those of aminothiazolyl cephalosporins, moxalactam, and aminoglycosides. The pharmacokinetics of norfloxacin were studied in six healthy volunteers, and three patients each with moderate renal and hepatic damage. A new specific and sensitive high performance liquid chromatography method was set up to measure plasma and urine concentrations of norfloxacin. Results in the patients with hepatic and renal damage indicated slight and not statistically significant differences in comparison with healthy volunteers. The pharmacokinetics and cantharides-induced blister fluid levels of norfloxacin were studied after a single 400 mg oral dose. After 24 h 27% of the administered dose was recovered in the urine as microbiologically active compound.
What trends antibiotics natural purchase cheap doxycycline line, challenges and barriers will impact the development and sizing of the Global Ciprofloxacin market? What are sales volume antibiotics z pack dosage cheap doxycycline online american express, revenue antibiotics given for sinus infection order doxycycline 100 mg free shipping, and price analysis of top manufacturers of Ciprofloxacin market? What are the Ciprofloxacin market opportunities and threats faced by the vendors in the global Ciprofloxacin Industry? With tables and figures helping analyze worldwide Global Ciprofloxacin market growth factors antibiotics for sinus infection during breastfeeding cost of doxycycline, this research provides key statistics on the state of the industry and is a valuable source of guidance and direction for companies and individuals interested in the market. Advancement in the technology has provided today’s businesses with multifaceted advantages resulting in daily economic shifts. Thus, it is very important for a company to comprehend the patterns of the market movements in order to strategize better. An efficient strategy offers the companies with a head start in planning and an edge over the competitors. Industry Research is the credible source for gaining the market reports that will provide you with the lead your business needs. This will allow your doctor to see if the medicine is working properly and to decide if you should continue to use it. Tell your doctor if you or your child are also using theophylline (Theo-Dur®) or other products that contain caffeine (eg, coffee, soda, chocolate). Ciprofloxacin may rarely cause inflammation (tendinitis) or tearing of a tendon (the cord that attaches muscles to bones). Serious side effects can occur during treatment with this medicine and can sometimes occur without warning. Stay away from rough sports or other situations where you could be bruised, cut, or injured. Exposure to sunlight, even for brief periods of time, may cause severe sunburn, skin rash, redness, itching, or discoloration. For example, if you are to take one dose a day, try to take it at the same time each day. For oral dosage form (extended-release tablets): For acute uncomplicated pyelonephritis: Adults—1000 milligrams (mg) once a day. If you miss a dose of the extended-release tablet and it is 8 hours or more until your next regular dose, take the missed dose as soon as possible, and then go back to your regular schedule. If you miss a dose and it is less than 8 hours until your next regular dose, skip the missed dose and take your next dose at the regular time. This high level of use, some due to misuse in the sense of unnecessary administration and consumption in irregular dose or with methods neither approved nor supervised by medical professionals, has been blamed for the rapid development of bacterial resistance against this drugs’ class [2, 4]. Ciprofloxacin is effective in the eradication of a wide spectrum of Gram-negative and some specific Gram-positive bacteria, including most strains of bacterial pathogens responsible for respiratory, urinary tract, gastrointestinal, and abdominal infections. The drug shows efficacy and safety in the treatment of adult patients with serious skin and soft tissue infections caused by a variety of bacterial pathogens [8]. Drug encapsulation and dosage reduction as a result of a site-specific approach is perhaps the most convenient way for controlled drug release. The goal of a drug delivery system is to provide the therapeutic dosage at the proper site maintaining the drug concentration during a specific release time. This requires not only a suitable material to hold the drug, and later release it, but also a biocompatible material, with high absorption rate and low rejection. The development of porous carriers had assisted drug delivery systems due to their properties of tunable pore size and well-defined surface properties, allowing a wide manipulation of the carrier in order to control the adsorption and release of drugs in a more reproducible and predictable manner [9]. In addition, the treatment of diabetic and phlebopathic ulcers with this membrane leads to a faster healing process due to a vascular growth factor found in the latex and due to a physical blockage of the entrance of new infectious agents in the treated site [10, 12]. The cream fraction after centrifugation was redispersed to make the desired 60% of dry rubber content latex and then washed twice by centrifugation to reduce the cytotoxic protein content on the solution. Typically the membranes were left for 2 days to fully polymerize at room temperature before use. For the release assay, latex membranes were placed individually in 200 mL of an aqueous solution, from which aliquots were collected during an interval ranging from 10 to 25,000 min. First-order equation occurs due to differences in concentration between the carrier and the media of release (Fickian diffusion) [21], Higuchi equation is applied to slightly soluble one-dimensional matrix that does not swell [22], and Hixson-Crowell equation is used when surfaces dimension diminishes proportionally but the initial geometry keeps constant [21, 23]. In vitro data were also fitted to Baker-Lonsdale equation, which describes the release from spherical matrices [21, 23]. When the release follows a non-Fickian release, a generic equation as Korsmeyer-Peppas equation can be used, where the value of the release exponent characterizes the release mechanism of drug from matrix [21, 22]. The membranes were characterized by X-ray powder diffraction, using a Siemens D5005 X-ray diffractometer and a graphite crystal as monochromator to select Cu Kα1 radiation (1. Results and Discussion Pharmaceutical innovation and research are increasingly focusing their attention on the development of delivery systems to enhance desirable therapeutic purposes while minimizing side effects [9, 24]. This calibration curve is important to establish a pattern between absorbance and the drug concentration. Using the calibration curve, a sample’s concentration can be derived by measuring its absorbance and then finding the corresponding -axis intercept. In contrast, the drug exhibits an X-ray diffraction pattern of a crystalline material with no amorphous component. The drug release depends mainly on the amount of encapsulated material (as a reservoir). After integration of these curves until 312 hours, the total amount of drug released by the membrane in 200 mL aqueous solution was 8. The parameters from each kinetic model equation are shown in Table 1, and the best fit is Korsmeyer-Peppas equation, due to its high coefficient of determination ( ). The release from a polymeric matrix is dependent on the solubility of the compound, erosion/degradation, swelling, and relaxation of the carrier [22]. In all spectra, absorption band from 3500 to 3450 cm−1 is due to the stretching vibrations of the hydroxyl group or the intermolecular hydrogen bonding. At 1705 and 1620 cm−1 the peaks are due to the stretching vibrations of the carbonyl group of carboxylic acid and ketone, respectively. The 1444 cm−1 peak is attributed to C–H bending or C–O, the 1271 cm−1 is due to C–C–C of ketone, and the 1045 cm−1 is due to C–F [27, 29–31]. Furthermore, functional groups of phospholipids and proteins have also been found at 1584, 1217, and 1036 cm−1 that are related to N–H bending, C–O, and –O–O–, respectively [28]. The overlapped band in the region of 3700–3200 cm−1 and the slight shift of the bands attributed to the carbonyl group indicate some interaction, most likely by hydrogen bonding, which were also observed on chitosan [29]. The new material became stiffer and brittle, with a smaller plastic deformation (less ductile). In this work, the method proposed by Langer and Folkman was used [35], that is, to mix the protein with the polymer (latex) in a colloidal state, in order to create a membrane that works as a delivery system. The controlled release of proteins is of interest for medical applications, since the dose can be adjusted according to the application envisaged. In addition, the X-ray spectroscopy technique shows that the drug did not interact chemically with the membrane. The use of lower drug doses and the control of drug delivery and site-specific release may improve the healing process and the quality of life of the patient and, in addition, can reduce the indiscriminate use of antibiotics. Further research is required to fulfill these predictions, such as in vitro studies focusing on the release rate and time and porosity required to achieve therapeutic effect and in vivo models to study the efficiency of the surgical bandage theory. Conflict of Interests The authors declare that they have no conflict of interests. Heitor Dias Murbach, Guilherme Jaques Ogawa, Bruno de Camargo Drago, and José Luiz Ferreira Cinman performed the experiments. Felipe Azevedo Borges, Matheus Carlos Romeiro Miranda, Natan Roberto de Barros, and Rondinelli Donizetti Herculano wrote the draft of the paper. In addition, the authors confirm that Rosângela Gonçalves da Silva and Alexandre Vinicius Guedes Mazalli had contributed to the paper. They contributed to the analyses of the mathematical model of the mechanism of release. In addition, Guilherme Jaques Ogawa and Rute Lopes had corrected the typographical and grammatical errors. Finally, the format of the paper has been updated by Matheus Carlos Romeiro Miranda, Rute Lopes, and Natan Roberto de Barros. Chronic bacterial prostatitis should be demonstrated by microbiological evidence localising infection to the prostate. Therapy with Ciprofloxacin Sandoz may be initiated before results of these tests are known; once results become available, appropriate therapy should be continued. For patients with complicated infections caused by organisms not highly susceptible such as Enterococcus faecalis, 500 mg may be administered every 12 hours.
Some patients for example those who have difficulty swallowing may find it easier to antibiotic biogram order doxycycline no prescription take Depakote Sprinkle Capsules because the capsules can be swallowed whole or The unit for the dosage strength is mostly expressed in mg milligrams and sometimes mcg micrograms oral antibiotics for moderate acne order doxycycline 100mg line. If you get the units right you put in the appropriate numbers and do the arithmetic antibiotic ingredients doxycycline 200mg low cost. Alternate each morning two tablets of ivacaftor 75 mg tezacaftor 50 mg elexacaftor 100 mg on the first day one tablet of ivacaftor 150 mg on the next day antibiotics metronidazole doxycycline 100 mg discount. The physician has ordered erythromycin nbsp the label on a bottle of Depakote tablets shows that each tablet contains 125 mg ordered atacand 16 mg po bid and on hand are atacand 8 mg tablets what is nbsp Depakote Tablets divalproex sodium Tablet strengths containing divalproex sodium equivalent to 125 mg 250 mg or 500 mg of valproic acid. Further, we demonstrated for the first time that this leads to increased hedonic food intake 50 minutes after the start of the infusion (although it should be noted that only a non-significant trend was found, which may be due to the late administration of the test relative to infusion, see below). We showed for the first time that the motilin receptor agonist, erythromycin, exerts its orexigenic effects by modulating the function of homeostatic and hedonic brain regions involved in the control of appetite and food intake, mediated by the brain-gut axis. Further, the differential response in these regions covaries with the increase in hunger ratings and predicts the subsequent increase in food intake after erythromycin versus placebo. Regarding the stimulatory effect of a low dose of erythromycin on hunger and prospective food consumption ratings, we confirmed previous work by our group7,8. In line with these effects on subjective ratings, there was a trend towards more hedonic food intake after erythromycin infusion compared to placebo, with a small effect size (Cohen’s d: 0. This effect may not have reached full significance due to the rather long interval between the infusion and the task (because of the primary focus of this study on brain responses). Hence, this needs to be confirmed in studies testing hedonic food intake at 30–40 minutes after the start of the infusion (i. Nevertheless, these results are in agreement with our previous work showing that healthy volunteers requested a soup meal more often after i. Interestingly, the responses in reward and homeostatic brain regions discussed below predicted the increase of hedonic food intake after erythromycin versus placebo infusion. Further, these brain regions mostly overlapped with the brain regions that covaried with the increase of hunger ratings. These findings indicate that the effect of erythromycin on reward and homeostatic brain regions mediated its hunger-inducing effect and therefore predicted the increase in hedonic food intake. We found enhanced activity after erythromycin administration in the hypothalamus, and this increase in activity covaried with the increase of subjective hunger and predicted the increase of ad libitum food intake after the erythromycin administration. Taken together, these findings suggest that the hypothalamus plays a key role in erythromycin-induced increases in hunger and food intake. In our study, we found associations between the differential brain responses in most of these mesolimbic reward system regions and the increase of hunger and prospective food consumption ratings after erythromycin versus saline administration, and the differential responses in these regions predicted differences in hedonic food intake. This indicates that not only an effect on homeostatic circuitry, but also on mesolimbic reward circuitry may be an important candidate brain-based mediator of the orexigenic effect of erythromycin. It should be noted that the direction of the responses differed between these regions, with some of them showing an increase in activity in response to erythromycin, and others showing a decrease. They suggested that the decrease was driven by the increase of circulating glucose and insulin. The exact gut-brain signaling mechanisms underlying the orexigenic effects of motilin and their neural basis had not been studied until now. In addition, old data indicate that erythromycin does only penetrate the blood-brain barrier to a very limited extent in a healthy population25. We were therefore not able to address direct correlations between erythromycin-induced gastric contractions and brain activity. The covariation we found between differential responses in these regions and subjective feelings (hunger, prospective food consumption) and eating behaviour (hedonic food intake) is in line with this interpretation. Moreover, it is probably also expressed on the vagus nerve as motilin increased gastric vagal afferent fiber activity in vitro in the suncus murinus28. This indicates that indirect (neural) or even direct (humoral) gut-brain signalling effects of motilin agonism cannot be excluded as a potential mechanism mediating the orexigenic effect of erythromycin on brain activity, in addition to motility-mediated effects described above. It is therefore likely that brain responses in different regions were mediated by different or multiple pathways with a differential lag. Given the observed erythromycin induced-effects on ghrelin, insulin, and glucose plasma levels and their covariation with the brain effects, these endocrine/metabolic effects may represent important alternative candidate neurohumoral gut-brain signals mediating the orexigenic effect of erythromycin. However, given the fact that hormone/glucose levels and brain responses are measured during the same timeframe, we cannot draw firm conclusion about the directionality of the associations, which renders the interpretation below inherently speculative. Ghrelin is recognized as a key orexigenic hormone, and has a structural resemblance to motilin29. The fact that erythromycin administration not only prevented the increase in ghrelin levels over time seen after placebo infusion, but even induced a decrease in ghrelin levels (compared to the pre-infusion baseline) in this study argues against ghrelin as the key mediator of the orexigenic effect of motilin agonism. Therefore, the decrease in ghrelin could rather be the consequence of a negative feedback mechanism resulting from the erythromycin infusion (through peripheral or top-down brain-gut signaling mechanisms triggered by the brain response to motilin agonism). An inhibition of the adrenergic pathway controlling ghrelin release might be a possibility30. We also found an increase of blood glucose and plasma insulin levels in response to erythromycin infusion. This is in line with our results showing an early peak (t = 20–30 min) in plasma insulin levels after erythromycin infusion. However, in our study we also found an increase of blood glucose together with an increase of plasma insulin after erythromycin infusion 2 hours after a standard meal. This can potentially be explained by the difference between fasted state and interprandial state, as erythromycin is well-known for being a prokinetic agent and hence improves gastric emptying31. In healthy humans, gastric half emptying time of a similar solid meal (250 kcal) varies between 20 and 118 min8. It is therefore possible that the increase in blood glucose levels after erythromycin infusion is caused by emptying of food remnants from the stomach into the small intestine. In this case, the observed increase in insulin levels after erythromycin infusion could be secondary to the increase in glucose levels. In addition, the change of blood glucose and plasma insulin levels covaried with brain responses in homeostatic and hedonic regions. Interestingly, there were some remarkable differences between the regions that covaried with glucose and those with insulin. These regions overlap with the regions that covaried with the change of blood glucose levels in response to erythromycin administration in our study. Not much is known about brain responses to exogenous insulin, as this requires a hyperinsulinemic-euglycemic clamp technique33. One possible explanation is that in our study, the increase of insulin was induced by erythromycin infusion, whereas erythromycin per se activated the hypothalamus. Therefore the covariation might be neutralized by the activation effect of erythromycin and the deactivation induced by glucose. More generally, it remains unclear whether the effects on glucose and/or insulin represent the true gut-brain signaling mediators of the observed orexigenic effect of erythromycin infusion, or are rather epiphenomena. As for ghrelin, the direction of the effects of erythromycin on glucose (increase) and hunger (increase) may argue againt a true mediating role, as, if anything, an increase in blood glucose would be expected to reduce hunger. To achieve a homogeneous sample and avoid potentially confounding sex differences, we only included healthy women, which implies the limitation that the present results cannot be extrapolated to men. In summary, the motilin agonist, erythromycin, increased hunger and hedonic food intake and attenuated the secretion of ghrelin in healthy female volunteers. Homeostatic brain regions, more specifically the hypothalamus, were activated in response to erythromycin infusion, and the activation of hypothalamus covaried with the increase of hunger and predicted the increase of hedonic food intake. Further, brain responses to erythromycin were also found in several key reward regions. These results confirm recent behavioural findings identifying motilin as a novel key orexigenic hormone in humans, and identify the gut-brain signaling mechanisms underlying its effect. Therefore, although further research is needed, we believe these results may inspire future drug development to improve dysregulation of appetite and food intake in patients populations characterized by loss of appetite and weight loss, including functional dyspepsia, anorexia nervosa and/or cachexia due to organic conditions. Without the appropriate and judicious use of these medications, many dogs would be much less likely to respond to treatment with environmental management and behavior modification therapy. Increase the dose of the medication if the typical maximum dose has not been reached and the patient has not shown undesirable side effects. In this article, we review the use of gabapentin in dogs for treating anxiety-related conditions.
Purchase on line doxycycline. Principles of Antimicrobial therapy- Part 1.