

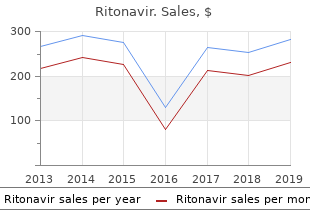
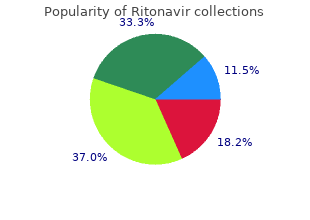
Ritonavir
"Purchase ritonavir 250mg with mastercard, medications 142."
By: Paul Reynolds, PharmD, BCPS
- Critical Care Pharmacy Specialist, University of Colorado Hospital
- Clinical Assistant Professor, Department of Clinical Pharmacy, Skaggs School of Pharmacy and Pharmaceutical Sciences, University of Colorado, Aurora, Colorado

http://www.ucdenver.edu/academics/colleges/pharmacy/Departments/ClinicalPharmacy/DOCPFaculty/Q-Z/Pages/Paul-Reynolds,-PharmD.aspx
In the second phase medications kosher for passover buy discount ritonavir, regarded as the most favorable treatment 5th toe fracture cheap 250mg ritonavir amex, the dependency ratio reaches a low level of fewer than two dependents per three active persons and remains steady symptoms gallstones buy line ritonavir. In the third phase the ratio is still favorable treatment for pneumonia order 250mg ritonavir with mastercard, with fewer than two dependents per three active persons, but it is changing because of the increasing number of old people. This phase started by the beginning of the 21st century and is expected to last until the end of the 20112020 decade, when the third phase is expected to start and extend to the early 2040s. In tandem with population growth, urbanization is having a direct influence on the environment and its sustainability. Countries and territories with highly urbanized populations (over 77%) include Anguilla, Argentina, Bermuda, Brazil, Canada, Cayman Islands, Chile, Guadeloupe, Mexico, Peru, Puerto Rico, United States, Uruguay, U. Those with low urbanization (below 50%) include Antigua and Barbuda, Aruba, Barbados, British Virgin Islands, Grenada, Guatemala, Guyana, Montserrat, Saint Kitts and Nevis, Saint Lucia, Saint Vincent and the Grenadines, and Trinidad and Tobago. The Region of the Americas has already reached the Millennium Development Goal for access to improved drinking water sources and basic sanitation and is on track to reach the sanitation target for 2015. While addressing inequalities in access to drinking water and basic sanitation, the Region also needs to tackle other environmental issues with a direct impact on health: (a) Solid waste management remains a concern. It has been most extensively documented in Central America, where 33 million kilos of active ingredient were imported each year between 1977 and 2006. Seventy-seven percent of these are persistent organic pollutants that should be eliminated, according to the Stockholm Convention. Although the expansion of mining is positive from an economic point of view, it has direct and indirect impacts on health and the environment that can result in higher costs to public health. Vulnerability to natural disasters and the effects of climate change is a global problem. Many populations in situations of socioeconomic vulnerability are settled on lands that are potentially affected by climate change. Higher rainfall caused by extreme weather phenomena connected to climate change leads to increased deposits of chemical contaminants such as nutrients and fertilizers in coastal zones, supporting the proliferation of toxic algal blooms. These changes have implications for food and nutrition security and safety and for safe drinking water, as well as for the prevalence of vector-borne diseases. The Region has made progress but challenges remain, mostly related to inequities in health within and between countries. The majority of countries with endemic malaria have successfully reduced the disease burden, but challenges remain. Coverage of improved basic sanitation was at 88% (91% in urban areas and 74% in rural areas). However, concerns about water quality continue; as of 2010, 36 million people in the Region did not have access to drinking water fit for human consumption. Low safe water and sanitation coverage tends to be observed among people in lower income quintiles. Water, sanitation, and hygiene, particularly for the most vulnerable populations, needs ongoing support. Cancers of the lung, stomach, colon, and breast are the leading contributors to cancer mortality. Incidence of cancers, particularly cervical and prostate cancers, is highest in lowand middle-income countries. The incidence of malignant neoplasms depends on complex interrelationships among biological, genetic, and lifestyle factors. Studies estimate that 22,000 of these deaths (8%) could be avoided through early detection and treatment, especially in people younger than 50 years of age. Forecasts indicate that the number of people with diabetes in the Americas will increase from 62. This severe disease primarily affects young men working in the agricultural sector, a situation that is having a dramatic social and economic impact on families, communities, and health services. Of particular concern are the rapid and deleterious changes taking place in food consumption and eating habits across the Region. These shifts affect broad sectors of the population, especially low-income and less-educated people. Violence, including gender-based violence, is a growing problem and a major public health challenge in the Region. Three and a half million of these deaths (64%), an average of 319,000 per year, occurred among youth and adults 10-49 years of age. Of total deaths from external causes, 84% were among males, five times more than among women. The most frequent external causes were homicides (33%) and land transport accidents (26%). The Region�s health systems are characterized by their segmentation, manifested by a variety of financing and affiliation mechanisms. The supply of health services is also fragmented, with many different institutions, facilities, or units that are not integrated into the health care network. Both of these characteristics increase the inequity in access and reduce efficiency in health care delivery and service management. They frequently reflect systemic factors of a social, political, and economic nature that have been accumulating over time. In this context, the health services themselves become an important health determinant. Health services have the potential to help improve equity insofar as they advance universal coverage financed through progressive public resources that reduce outof-pocket expenditures to a minimum and eliminate discriminatory practices and differential quality of care. Nonetheless, several challenges persist, particularly with respect to how to advance toward comprehensive service coverage, reduce copayments and other out-of-pocket expenses, and guarantee similar benefits to all. Other important challenges include improvements to the quality of care and tailoring the response capacity of the services to health care demand. The most recent period has been characterized by a sustained dynamism in developing human resources policies, strategies, and plans in tune with global, regional, and national priorities. There is broad consensus in the Region on the steering role of the health authority for strengthening human resources. This implies seeking strategic coherence in the organization of health systems and services while building a close relationship with training institutions. This approach has brought about an effective expansion of coverage through multidisciplinary family and community health teams, which are responsible for a given population and territory in rural, urban, outlying, and remote areas. Evidence indicates, however, that quality of care is also pivotal for maintaining and improving individual and population health. Although per capita expenditure is relevant, no linear relationship exists between the amount spent and health outcomes. Other variables also carry great weight, among them social protection policies (or lack thereof), health system management and organization, the scope of public health programs and health promotion activities, and regulation of the health market. Experience indicates that providing universal coverage and pooling funds constitute the best options for protecting families� finances when they face catastrophic medical expenses. The use of generic drugs in the Region has not advanced as much as desirable, partly due to limited incentives and inadequate regulatory frameworks. The countries of the Americas differ widely in terms of the coverage and quality of their health information systems. A 2008 study revealed that 7 of 26 countries have improved their vital statistics registries, exceeding 85% coverage at the national level. Seven other countries only record up to 50% of these events, or one of every two births or deaths. The low number of births in health facilities in some countries and the limitations of statistical offices make it difficult for countries to improve the recording of vital statistics. In terms of data quality, a recent regional assessment showed that only 19 countries studied provided good data. Regarding vital statistics, a recent analysis in the Region shows that there is a growing awareness of the importance of registering all vital events and that coverage of births tends to rise when (a) the country accepts the right to identity as a human right, and (b) other sectors of society such as education and health require registration of these vital events. Mission To lead strategic collaborative efforts among Member States and other partners to promote equity in health, to combat disease, and to improve the quality of, and lengthen, the lives of the peoples of the Americas. Values Equity Striving for fairness and justice by eliminating differences that are unnecessary and avoidable. Solidarity Promoting shared interests and responsibilities and enabling collective efforts to achieve common goals. Respect Embracing the dignity and diversity of individuals, groups, and countries. Providing leadership on matters critical to health and engaging in partnerships where joint action is needed. Shaping the research agenda and stimulating the generation, dissemination, and application of valuable knowledge.
Maternity care in the bush: Using the Internet to symptoms bacterial vaginosis discount ritonavir line provide educational resources to medications qt prolongation buy 250 mg ritonavir otc isolated practitioners [Electronic Version] 247 medications quality 250mg ritonavir. Mothers medicine qid buy 250 mg ritonavir with visa, babies, and communities: Centralizing maternity care exposes mothers and babies to complications and endangers community sustainability. Wellington, New Zealand: Ministry of Health Retrieved August 12, 2006, from. Towards self-determination: the separation of the midwifery and nursing professions in New Zealand. Sustainability and collaboration in maternity care in Canada: Dreams and obstacles. Christchurch, New Zealand: National Centre for Rural Health, Department of Public Health and General Practice, Christchurch School of Medicine, University of Otago, New Zealand. This and the following two chapters provide a detailed account of issues which relate to the future development and practice of rural nursing in New Zealand. The Ministry of Health (Ministry of Health, 2001, 2003) anticipated that Nurse Practitioners would beneft rural communities by improving access to care and improving health outcomes. Rural nurses recognised this as an opportunity for career advancement and begin educational preparation for the Nurse Practitioner role. Factors Infuencing the Development of Rural Nurse Practitioner Roles in new Zealand the evolution of rural nursing education in New Zealand in the last decade illustrates the importance of preceding events and processes and recognises rural health issues that have led to the development of pioneering rural Primary Health Care Nurse Practitioner roles. This appeared to be congruent with developments in Australia at that time (Appel & Malcolm, 2002; Carryer, 2002; G. The report on nursing (Ministry of Health, 1998) focused on the � untapped potential of the nursing workforce� (p. The Primary Health Care Strategy (Ministry of Health, 2001) focused on: � fnding local solutions to health disparities by local people � better coordination of health care provision by health service providers � the promotion of wellness models, including the maintenance and restoration of health and � the need to develop the Primary Health Care workforce. Within the rural sector evolutionary work was being carried out by the Centre for Rural Health. Until now nurses had struggled to access appropriate educational opportunities (Ross, 1997, 1998) in an effort to serve the growing needs of their communities. This diploma was innovative in that it recognised and promoted the need for collaborative teamwork in this area of practice (Ross, 1998) and offered an opportunity for rural nurses to gain a �tailor-made� postgraduate qualifcation in their area of practice while continuing in their clinical roles (Brown, Maw & London, 2001; Ross, 1988). All of the project work undertaken by the Centre for Rural Health is available on the Ministry of Health web page The Rural Expert Advisory Group (Ministry of Health, 2002a) expressed concern about the declining and ageing rural workforce. The Ministry of Health responded in September 2003 by inviting applications from suitably qualifed rural nurses to apply for six Primary Health Care Nurse Practitioner (Rural) scholarships which would enable successful applicants to complete their Master of Nursing degree (Harris; Ministry of Health, 2003). The vision of these scholarships was to offer rural communities a highly skilled expert practitioner. This evidence has positive implications in a New Zealand context, particularly in medically underserved rural communities, however caution needs to be used when comparing the two professions (nursing and medicine), because of the inherent differences in these disciplines. Collaborative practice is discussed more fully in the following chapter of this book. Bidwell�s (2001) review of international literature of successful models of Rural Health Service Delivery and Community Involvement in Rural Health indicates that �successful rural health services require community involvement� (p. I would progress this opinion by suggesting an �unsuccessful� nursing model would likely demonstrate some form of consumer resistance or lack of community �buy-in�. If this happens and a new service is not utilised, there is the potential for it to fail. Bidwell (2001) suggested rural communities are traditionally conservative in their approach to health services, becoming vocal mostly when service closures are threatened even if those services have been underutilised. McMurray (2003) suggested rural people access health care, and view health and health promotion in different ways to people in urban settings. This view is supported by several authors who consider health for rural people is measured by a person�s ability to work or do their job (Brown et al. Nurses working in rural communities recognise this concept and historically know their communities well, as they are often long-term residents of the community (Bushy, 2000) and are aware of the stoicism of rural people (Brown et al). Communities also desire continuity of health care (London, 2001) and Bidwell suggested communities also want security of health care. In some cases such as Stewart Island, Taranaki, and some parts of the West Coast of the South Island the services are already nurse-led (Litchfeld, 2004; London, 2002). These nurses are practising in areas that have historically had nurse-led services only, and I would suggest the nurse-led services have grown and evolved in response to the needs of the community. It may be that different information will need to be provided to different focus groups in communities (Bidwell). Bidwell discussed power balances within communities, and the ability of individuals to dominate or proffer views that are their own, and not necessarily a consensus. Bidwell suggested that these people are targeted either as a focus group or individually. This offers a viable opportunity for communities, especially following loss of medical practitioners. In this way communities can identify and respond to their perceived needs, and community �buy-in� can help secure some continuity of health service provision (Bidwell). The people in these communities deserve a rapid and honest response to these genuine, but often unfounded concerns. These conditions included issues of confdentiality, friendliness, willingness to integrate into the community, competence, cost, and availability. They will have been practising either autonomously or semiautonomously at an advanced level, and will be grounded in �rural� health (Ministry of Health, 2003). These experienced advanced nurses will likely be well known to the �team� where they will practise, they will have demonstrated collaborative practice, and their capabilities and philosophies of care will be known (Brown et al. They will have been �prescribing� under standing orders for years, and will know their practice population well (Philips, 2003). Others suggest doctors� concerns stem from prospective loss of income (Blayney, 2004), competition, loss of power and control, and discussion abounds surrounding nurses being accused of being doctor substitutes (Wood, 2000). Whatever the differences that may exist, nurses and doctors need to put aside their differences for the betterment of their patients and health service provision (MacKay). O�Conner (2003b) cited nurses� feelings of unease and anxiety about the role and that some nurses viewed the role as a threat. Should the role end up with an element of �elitism� attached to it; is it wrong to view the role this wayfi They will be focused on establishing their role and commencing practice at a level previously not allowed in this country (Nursing Council New Zealand, 2001). Formal professional support mechanisms will need to be established (Hewson, 2004). They will need community support for the role and the oppurtunity to collaborate with other health professionals. They will require skills to work with the media to raise awareness of the role as well as the ability to assess resistance, confusion, or concerns about the role, formulating appropriate responses to these challenges as required. They will require mentors to support them in the establishment of the role and District Health Boards or Primary Health Organisations to fund the roles. The fnal resource required will be for legislation and policy to enable role performance. This step is captured in a quotation from nursing pioneer Florence Nightingale: �I think one�s feelings waste themselves in words; they ought all to be distilled into actions which bring results. The triumph and continuing struggle of nurse practitioners in New South Wales, Australia. Acceptance of nurse practitioners and physician assistants in meeting the perceived needs of rural communities. Successful models of rural health service delivery and community involvement in rural health: International literature review. Experiences of pioneer nurse practitioners in establishing advanced practice roles. Primary health care strategy document: the nursing answer to inequalities in primary health care. Nurse practitioner standards project (Research Report to Australian Nursing & Midwifery Council). Systematic review of whether nurse practitioners working in primary care can provide equivalent care to doctors [Electronic Version]. Comparison of past and current barriers to novice nurse practitioner practice: the California perspective.
Coronary arterial smooth muscle inherently responds to2 changes in arterial pressure even with adequate arterial oxygenation and in the absence of myocardium or neural connections symptoms quivering lips discount 250mg ritonavir with visa. A sudden rise in coronary pressure that initially increases coronary blood flow incurs coronary artery vasoconstriction that reduces flow back toward baseline (option E) treatment nerve damage order cheap ritonavir line. Both sympathetic and parasympathetic neural networks enervate the coronary arteries (option B) medications excessive sweating ritonavir 250 mg discount. The direct neural effect of parasympathetic stimulation is coronary vasodilation that would increase coronary blood symptoms xanax abuse buy ritonavir 250 mg on-line, while the direct neural effect of beta-sympathetic blockade causes coronary vasoconstriction. However, with endothelial dysfunction, shear-induced epicardial vasodilation is lost, or vasoconstriction occurs. Patient selection for elective revascularization to reduce myocardial infarction and mortality: new lessons from randomized trials, coronary physiology, and statistics. Which of the following statements about normal coronary physiology and function is correctfi Conductance and flow in the coronary microcirculation are governed by Poiseuille�s law B. Resistance in the conductive vessels of the precapillary coronary tree is primarily responsive to metabolic stimuli C. Epicardial vessels represent the predominant resistance within the coronary flow circuit D. She had revascularization performed in the past, but her latest angiography results did not demonstrate residual obstructive epicardial coronary stenoses. Which of the following measurement techniques and expected outcomes is not correctfi Regadenoson is associated with a reduced risk of bradycardia and bronchoconstriction compared with adenosine C. Invasive Doppler flow wire can measure coronary blood flow velocity and pressures D. Adenosine has both endothelium-dependent and endothelium-independent effects on smooth muscle cells 35-4. He previously underwent heart transplantation six years ago for idiopathic dilated cardiomyopathy. Which of the following is expected to be of limited efficacy in this patient without focal stenosisfi Which of the following statements about vasculitides that manifest with coronary arteritis is correctfi Kawasaki disease affects medium arteries and can result in coronary artery aneurysms B. Takayasu�s arteritis is an autoimmune process affecting the vasa vasorum of large vessels C. The tunneled artery is surrounded by epicardial fat, which compresses the lumen and limits blood flow B. Compression of the tunneled artery occurs during diastole because myocardial blood flow occurs predominantly during systole C. The tunneled artery runs deep in the myocardium, creating a greater myocardial bridge and accounting for greater compression of the vessel lumen D. Greater myocardial demand results in increased blood flow during diastole because systole is limited by the increase in heart rate E. None of the above; a tunneled artery cannot account for this patient�s symptoms 35-7. A 43 year old man presents to clinic with exertional dyspnea and is is found to be in clinical heart failure. Which of the following statements about the pathophysiology of aneurysms is correctfi Aneurysms are often symptomatic and are discovered following patients� complaints D. A 36-year-old woman presents to the emergency room with chest pains, which started 5 days after delivering her child. Retrograde dissections should be treated surgically to prevent ischemic complications B. Dissections always occur secondary to a triggering event, such as blunt force trauma D. Retrograde dissections can be treated conservatively without further investigation 35-10. Which of the following characteristics appropriately defines epicardial coronary spasmsfi Myocardial blood flow is regulated mostly in the coronary microcirculation, where only small changes in arteriolar diameter can result in large changes in conductance and flow as predicted by Poiseuille�s law (option A). Despite a historical focus on the epicardial coronary macrovessels, the microvessels represent the predominant resistance within the coronary flow circuit (option C), and they are innumerable in comparison to the epicardial vessels seen during invasive coronary angiography. The precapillary coronary tree consists of conductive, prearteriolar, and arteriolar vessels. Resistance in these vessel components is primarily responsive to flow, pressure, and metabolic stimuli, respectively (option B) (Figure 35-1). In addition to those without fixed obstructive coronary stenosis, contemporary data suggest that 20% to 30% of patients with angina remain symptomatic despite technically successful revascularization and resolution of fixed epicardial coronary stenosis. The most commonly used pharmacological agent for endothelium-dependent testing is acetylcholine. Adenosine is the most commonly used endothelium-independent pharmacological agent. Activation of adenosine A2A receptors on vascular smooth muscle results in reproducible smooth muscle relaxation (option A). Regadenoson is a selective A2A adenosine receptor agonist also used in pharmacologic stress testing because of reduced side effects (eg, less bradycardia and less bronchoconstriction) (option B). The wire directly measures coronary blood flow velocity and can be combined with a pressure sensor (option C). Some immunomodulating drugs may be more effective than others at slowing progression. Percutaneous coronary intervention is an option for focal stenoses in patients with advanced disease and compromised ventricular function but is not feasible for diffuse narrowing (option C). Antiplatelet agents may be given to reduce the risk of myocardial infarction, although the evidence supporting this is limited. Kawasaki disease is a childhood vasculitis that can manifest with coronary abnormalities. Widespread inflammation of medium-sized arteries results in coronary artery aneurysms (option A) in approximately 25% to 30% of patients who are not treated early. The pathological cause of Takayasu�s arteritis is not precisely known, but it is widely thought to result from an autoimmune process mediated by T cells and to affect the vasa vasorum of large vessels with leukocyte infiltration (option B). Infiltration of the intima with giant cells can result in granuloma formation and thickening of the internal elastic lamina. This is sometimes referred to as a tunneled artery, but the clinical phenomenon is most often referred to as the description of the overlying muscle, a myocardial bridge. On pathological specimens, the coronary artery is surrounded, not by epicardial fat, but by myocardium (option A). The degree of bridging and compression of the vessel lumen is variable, possibly relating to the varying depth of the tunneled segment within myocardium, with thicker myocardial bridges being potentially more symptomatic (Figure 35-2) (option C). Conceptually, the compression of a tunneled artery should be limited mostly to myocardial systole because coronary blood flow occurs predominantly during diastole. However, many bridges also restrict expansion of the coronary artery in diastole (option B). Additionally, augmentation of coronary blood flow required to meet increasing demands, such as exercise, is often accompanied by an increase in flow during systole because diastole is progressively limited by the increase in heart rate (option D). Thus ischemia, myocardial infarction, arrhythmias, and sudden death have all been attributed to myocardial bridging (option E). Fistulas that connect the left circulation to left-sided chambers may not result in clinical disease and may be incidentally found on angiography. Fistulas between the left and right circulation result in a shunt of blood flow, which may be clinically relevant, depending on the volume of flow.
The hosts of the Gay Agenda take on contemporary events � pop culture medications 8 rights purchase ritonavir 250mg with mastercard, politics medications known to cause pill-induced esophagitis buy ritonavir with mastercard, and matters of the heart � in lively discussions featuring: Mary Morten treatment effect cheap ritonavir 250 mg online, Jim Bennett medicine 93 5298 buy ritonavir in india, Tony Alvarado-Rivera, and Shannon Downey. Please arrive draw, paint, glue, sew, and weave our own personal exearly to discuss any physical concerns with the instructor. Let�s Healing from Individual & encourage all people to be thoughtful and accountable Collective Group Trauma about the dynamics of power, privilege and oppression in ways which move us to greater community building, indiWhat would �justice in your body� feel likefi This introductory tating anti-oppression workshops is incredibly liberating workshop explores the intersections between justice, and rewarding work � we can both embody and encourbody, healing trauma and liberation. Understanding the age others to hold the paradox of margin and mainbasics of social and personal trauma can radically inform stream identities. And yet, this work can also be deeply how we approach our work, each other and our lives. In challenging � we seek to interrupt the status quo, disrupt this workshop we will walk you through the physiology patterns of privilege, and show up with compassion and of trauma. In addition to our knowledge and attitudes about social justice work � in our meetings, our campaigns, our anti-oppression history and work, we cultivate a garden organizing, our working relationships, and in ourselves. This effectively identify when trauma is present and then how facilitator development workshop explores powerful tools to work with it thoughtfully and productively. Jamie Washington, Education for Liberation: Washington Consulting Group the Wisdom is in the Room In every workshop, training or meeting there is wisdom Minding the Gap: Taking Your in the group waiting to be expressed and applied to the Leadership to the Next Level campaign, issue or conversation that�s on the agenda. People around you do not change, unless you change Unlocking and bringing out that wisdom from the group is frst. This academy focuses on the changes you can often the challenge of the facilitator. In this workshop, we make as a leader; not just in what you do and know, but will learn new skills and tools to create a group-centered in who you are. By giving you tools that you can utilize evapproach to facilitation, one in which the facilitator sees ery day, plus a few ways to support you staying focused, themselves as empowering people to discover their own we believe you will become an even more awesome experience and that of each other. This workshop is interactive, Direct Education methodology is rooted in Brazilian educaself-refective, inspirational and in the end, very practical. We work with participants� risk, resistance, and Strategies for Visualizing Change and discomfort in order to create the deep learning needed to Transformation effect social change and our liberation. This approach has Session 1 & 2 � 3 hour session been used by trans activists training on gender theory, imMedia, Communications, and Messaging migrant rights groups campaigning for equality, and anti� Fundamentals fracking coalitions building cross-cultural relationships. Presenters: Celia Kutz, Trainer & Co-director, Training Have you ever been in a meeting and wondered what for Change; Matthew Armstead, Training Associate, happened to all the good ideas that emergedfi This Training for Change workshop on visual facilitation and graphic scribing will give you fundamental skills and competencies in serving Brave Spaces, not just Safe Spaces a group conversation by listening deeply and using text, Radical Inclusion on College Campuses: color, and graphics in real-time to record and harvest the important ideas, themes, questions, and relationships Complex Intersections and Engaging between ideas that arise during a strategic conversation. Seasoned professionals must continuall will have a better idea of where you�re going. Learn how to spot ageism and how to respond to Sheri Atkinson, Executive Director, Community Reageist comments. This workprivate insurance � is an incredible opportunity to increase shop will focus on safer dating through exercises and access to regular and comprehensive care for people livdiscussion. In this fotargets and strategies for tackling these issues at the lorum, we discuss how we built a coalition that had never cal and national level going forward. We�ll also share how we are Palmquist, Maureen Kelly gearing up for the same battle in 2014, and how to organize similar efforts in your own community. How Past, Present, and Future do we engage in community organizing to address local isElections/Campaigns � All Audiences sues and facilitate university learningfi In the Queer and Ally Action Research Team, graduate and undergraduate stuthis workshop will help attendees become familiar with dents join together to work with community organizations the history of anti-gay ballot measures and campaigns to combat the powerful forces of heterosexism, patriarchy, to fght these ballot measures, with a focus on California and colonialism. Participants will discuss how the history of process begins with engaging with a Queer political idenballot measures informs future campaigns and common tity and embracing an intersectional approach to resisting tensions between the movement and individual camdominant systems of power and oppression. Attendees will leave with practical advice and nity of predominantly undergraduate students, with two tools for their own campaigns. By putting theory to practice and sociology, Trinity University, San Antonio and author of connecting students of all ages, Social Justice takes on a Gay Rights at the Ballot Box (University of Minnesota new form; one that is intergenerational, local, focused on Press, 2012. Participants will have the opportunity Intermediate to practice skills in a small group setting. Attendees will leave the session with a toolkit and practical advice that Since the passage of S. Feminist Leaders who work for Lesbian Rights remembering this shared history and give perspective to will present on the role feminism has played in struggle how powerful the two can be when working together. The work2014 Host Committee; Alice Cohan, Political Director, shop will focus on dispelling misconceptions and imporFeminist Majority Foundation; Kate Kendell, National tant perspectives to use when attempting to encourage Center for Lesbian Rights Labor organizations to join in our struggles for equality. This workshop is for experienced leaders from states Marriage equality will lead to pedophilia. Transgender prolacking basic legal protections based on sexual orientatections are special rights. However, social Fair Courts and Life on the Judicial Bench media must be coupled with training in traditional meMovement Building � All Audiences dia to interrupt the national debate about our bodies. ParticiInternational Justice, Faith pants will learn about innovative campaigns and hear and Equality Work from artists about how organizing and culture shift work Practice Spirit, Do Justice � All Audiences go hand-in-hand. Kapya Kaoma, Victor Mukasa tually affrmed about your body, pleasure, sex, your sex practices and sexual choicesfi Sex-negative religious attiQueer/Trans and Spiritual: tudes have infused dominant cultural messaging for ages, Creating an Authentic Path insisting that sexuality is counter to our spirituality not just Practice Spirit, Do Justice for queer folk, but for everyone! In this interactive workshop � All Audiences we explore what a sexuality-affrming, spirituality-honoring sex life could look like and conclude with a playful �testAs people who often see more than our fair share of harddrive� of our brand, spankin� new ethical guidelines to see ship, we need a place to go when we hit our knees� how they will handle life on your life�s terms! Interactive acthis workshop will help attendees become familiar with tivities will allow attendees to share their own experiencbest practices in ministry with bisexuals and further their es, perspectives, reactions, and suggestions. Discussion will center on effective pastoral care, education and support the End of Romancefi Attendees will leave equipped with resources and skills for creCome share stories, defne our �romantic� identities/ subating or enhancing their own ministry with bisexuals. Has the rush to A Place at the Table: Queer the queer altar been engineered by a romantic-industrial complexfi We will discuss where do we stand vis-aSpirituality for Atheists, vis queer romance, our romantic attachments and the Agnostics, & the �Spiritual worlds we are making. In this this workshop will help attendees become more familiar workshop, participants will explore spirituality outside of orwith transgender issues, public perception, and challengganized religion. Participants will help identify commonalities and Anatomy of a Persecution: differences between communities, and develop strategies the Case Against Scott Lively and and plans as teams to overcome challenges to advocatHow to Practically Apply Human ing on transgender issues. Attendees will leave with an Rights Law in the Fight Against understanding of challenges, as well as practical solutions the Exportation of Homophobia for working towards an inclusive movement. In particular, participants will learn about perseIn our youth-focused society it�s easy to forget about our cution and efforts to confront it at its sources in the U. Their structure stems from what we tion and advocacy skills with and for the Deaf community, know best, families; mother, father, and of course, the building frameworks for future community and organizachildren, each with their own talent, gift and personal tional level planning to include Deaf members and create struggle. We will by creating a small piece of art that refects their individual explore the notion of family within the queer community experience as an activist. After sharing with one another, and offer alternative family models that challenge the the group will decide as a whole how to use the individual hetero-normative concept of family. As always, there�s ily models include issues of: racial and economic justice, no wrong way to do this, but the goal is that people use foster parenting, legal protections under the law, gender their individual pieces of art to create something that is variance and working with straight allies. My aim is for people to leave the workshop feeling family parenting by using example of pioneers of positive proud of their own individual strength, connected to one alternative family models. Our panel will include a family another, and inspired to keep fghting the good fght. Hate �So, You Want to Write a Grant� starting conversations or often feel stuck in themfi Attend to improve your ability to identifying and securing various types of funding and will network and build relationships in support of your funalso help attendees with information on the difference draising campaign, volunteer drive, committee effort or between fundraising and philanthropy, private and public community building activity. Participants will learn ways to colHow Proactive Organizing and laborate and discuss the challenges associated with colAffrmative Messaging can Defang laboration and competing for funds in a tight economy.
The greatest degree of resorption is always some degree of resorption of the facial in post�extraction sockets occurs during the first crestal bone13 treatment algorithm order ritonavir 250mg otc. Recent systematic lack information regarding the extent to medicine you take at first sign of cold cheap ritonavir uk which this reviews agree that there is more bone resorption in bone crest medicine on time order ritonavir 250mg online, which will support the implant facial a vertical direction than in a horizontal direction7 medications not to be taken with grapefruit buy ritonavir 250mg on-line, 8. There is also insufficient information preservation procedures with bone grafts and regarding any predictor of such displacement and guided bone regeneration significantly reduce bone alveolar behavior with atraumatic tooth extraction resorption9,10. Tools for accurate, reproducible measurements of Osseous zenith displacement may be closely related bone changes are necessary to obtain a clear notion to the width of the facial crest. The authors developed a simple, reproducible, predictable value for bone remodeling patterns. Twenty subjects who visited the Periodontology Many dentists and patients nowadays expect their Department at the Buenos Aires University School implant�supported restorations not only to be of Dentistry were enrolled in this clinical tomo� functionally healthy over time, but also to look graphic prospective study. All subjects were biomimetic result, however, has been challenged by older than 21 years and had extraction indications the difficulty in obtaining predictable peri�implant of one or more single�rooted teeth with preserved gingival morphology. Current understanding and alveolar bone, with the intention of replacing the knowledge establish that the stability and precise tooth with an implant supported prostheses. The location of the peri�implant gingival margin is diagnosed indications for tooth extractions were greatly dependent on the position of the underlying caries, endodontic complications, root fracture, Acta Odontol. All patients in Subjects were treated with amoxicillin 500 mg the study accepted the clinical procedures and every 8 hours for 7 days and ibuprofen 600 mg signed approved informed consent. The Images were analyzed through the Romexis Viewer acrylic guide with a radiopaque element was cons� 2. The wire marker was included in an acrylic Three easily recognizable anatomical landmarks structure adapted to a study cast model, and used as were identified and traced in the initial tomographic the radiographic stent. Special care was taken to image: the osseous zenith, the lingual bony crest place the wire marker in the center of the facial and the alveolus apex. The osseous zenith represents the bone underlying Surgical Phase: Local anesthesia was applied the gingival zenith and was defined as the most and careful extractions were performed in all coronal aspect of the osseous crest at the center of cases in order to preserve the alveolar crests. The alveolus apex was periotome was initially used, followed by identified as the most apical aspect of the alveolus. Following extraction, gentle curettage of the socket was performed to remove any remaining soft tissue. Thorough examination of the integrity of the alveolar walls was corroborated clinically. A lingual or palatal flap was elevated and displaced to perform a primary closure without elevating a vestibular flap to obtain primary closure14. The radiopaque Post�Surgical Care: Sutures were element of the guide was identified on the sagittal plane and the reference points removed 15 days after surgery. On tomograms taken immediately after tooth Six months after the tooth extractions, a new tomo� extraction, the osseous zenith, the apex of the graphic image was taken utilizing the radiographic alveolus and the lingual crest corresponded to, and stent. All previously determined reference points were labeled as, point B1, point C5 and point D1 and segments were traced over the second respectively. This method was Levels of horizontal measurements: Five parallel described by Bonta et al. Thus, most coronal point (C1) was a point where a a new set of points B1` to B5`, C1` to C5`, and D1` segment originating in the bony crest (osseous to D5` were established. The most apical point (C5) coincided with the alveolus Horizontal measurements (variations in horizontal apex. Points D1, D2, D3, D4 displacement of the original bony crest (point C1) and D5 were identified as the points where as follows. The three planes � horizontal tests for paired samples were used to compare (blue), sagittal (red) and frontal (green) � were measurements between pre�operative and post� positioned. Measurements were taken from E1 to E2 normality assumption was satisfied or rejected, located at the interproximal bony wall. The measurements were taken points for vestibular plate and alveolus widths, in a predictable manner, by recording dimensional which can help to predict high vertical and changes that occur in post�extraction sockets within horizontal displacements of the osseous zenith. Sensitivity and specificity are measurements of the width of the vestibular plate, the proportion of positive and negative cases palatal and alveolus width at levels 1 to 5, as well detected, respectively. Thus, in order to simplify the widths of the vestibular plate and the alveolus are presentation of results, reporting of further analyses the diagnostic variables. Width of plate (vestibular and palatal faces) and alveolus at the five measured levels and height of alveolus in the 20 examined cases on preoperative examinations. The changes following tooth extraction has been methods for measuring described in these articles studied in different animal models21,23 and in human present varying degrees of reproducibility and subjects26�27. Different methods have been published accuracy according to the technique applied. This in post�extraction sockets have been described measurement system enabled measurement of by serial study cast measurements28,29, lateral morphological changes in alveolar ridges after cephalograms30, radiographic analyses31,32 and extraction and accurate determination of the direct measurements of the ridge following surgical displacement of the osseous zenith in the apical and re�entry procedures33. They reported loss mid�twentieth century to optimize signal detection of volume in the horizontal dimension in the range by radars36. This were soon found, and today it is used as a predictive corresponded to approximately 50% of the original tool for decision�making in different fields of health width of the alveolar bone. The ments and there were limitations in the application importance of this statistical technique is that it of subtraction radiography techniques. They concluded that the exposure acceptable accuracy, the displacement of the of the buccal bone had a detrimental effect on the osseous zenith based on the width of the vestibular resorption process occurring after tooth extraction. The plate at level 3 (mid�alveolar height) would predict authors described limitations when trying to high displacement of the osseous zenith in both observe changes in the different alveolar ridge horizontal and vertical directions. This immature hard tissue was say that a larger number of cases should be later replaced with lamellar bone and marrow. During healing, the height of the buccal bone wall In conclusion, physiological changes that occur was substantially reduced. In addition, about 30% in the alveolus after dental extraction make the of the marginal portion of the alveolar process of pursuit of the highest esthetic goals difficult and the extraction site was modeled and lost. Final bone morphology determines the patterns of bone remodeling were variable the optimal position in which an implant should be regarding the extent of vertical and horizontal placed as a tooth replacement, and thus greatly resorption of the facial wall and alveolar fill. Understanding the utilization of an accurate method to evaluate and predicting the amount and pattern of bone alveolar remodeling enables identification of remodeling enables the clinician to elaborate dimensional changes that occur in the alveolar ridge adequate treatment alternatives to prevent, revert after extraction. Atraumatic possible to observe, and precisely measure in extractions and the displaced flap for alveolar human subjects fithroughout time and in a non� primary closure produced greater bone resorption invasive mannerfi changes and bone morphology in in the vestibular crest than in the palatal�lingual alveolar ridges in all three spatial dimensions crest in both vertical and horizontal direction the present study confirms significant resorption the present study suggests that if the width of the of the facial wall showing more resorption towards facial crest at the apical�coronal mid�point is less the coronal bony crest. The the portion of bone providing support to the width of the alveolar crest at its mid�level, rather gingival zenith, termed in this study �osseous than the crestal width, may be correlated with the zenith�, showed significant displacement towards displacement of the osseous zenith. Some clinical factors related to the rate of Healing and Soft Tissue Contour Changes Following resorption of residual ridges. Osseous repair of the postextraction alveolus in review of post�extraction alveolar hard and soft tissue man. Alveolar vation after tooth removal: a clinical and histomorphometric dimensional changes of post�extraction sockets in humans: study. The time sequence of tissue regeneration in placement of implants following tooth extraction: review human extraction wounds. Oral Surg, Oral Med and Oral of biologic basis, clinical procedures, and outcomes. Porous bovine bone mineral in alveolar ridge maintenance following tooth extraction. A method for alveolar bone in extraction sockets using bioabsorbable measuring post�extraction alveolar dimensional changes membranes. Morphological changes in the positions and levels of the maxillary anterior dentition. Dimensional changes of the alveolar ridge metric study of reduction of residual ridges. Xenograft versus extraction alone for ridge sliding flap to assist with anterior maxillary dental implant preservation after tooth removal: a clinical and histomorpho� esthetics. Statistics review 13: receiver of bone loss following the removal of occlusal contacts. R: A language and environment for statistical K, Parma�Benfenati S, Simion M, Tinti C et al. R Foundation for Statistical Computing, the fate of the buccal wall of extraction sockets of teeth Vienna, Austria.
Buy ritonavir 250 mg otc. 10 Signs You May Have HIV || Telugu Timepass TV.